Ultrasound of the Week #043
Case:
A 9 year old male with known sickle cell disease (SCD) presented with a 4 day history of pain in his central chest and left side. This was constant, not pleuritic and with no radiation. In department after home analgesia of paracetamol he reported it as 7/10 severity. He did not feel breathless, had no cough and denied fever at home although was febrile in department.
Obs: SpO2 94% on room air, mild increased work of breathing, RR 24, HR 92bpm, Temp 37.8.
Meds: Penicillin V, Folic acid
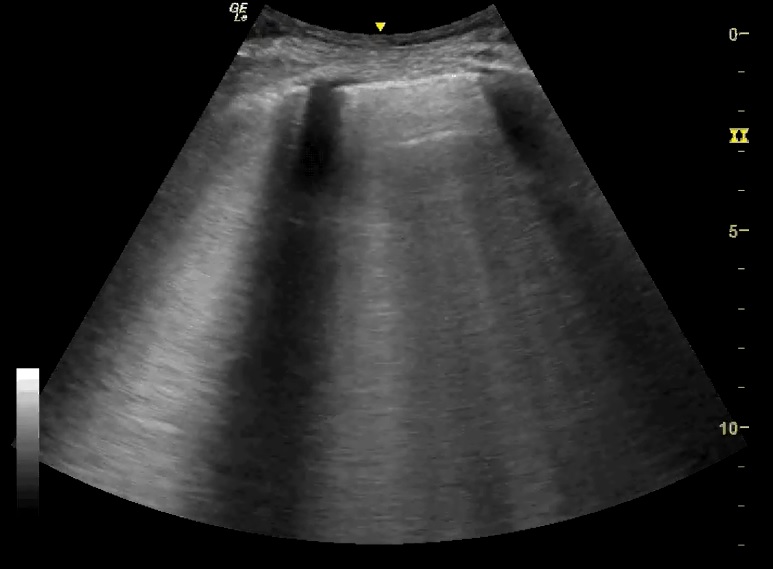
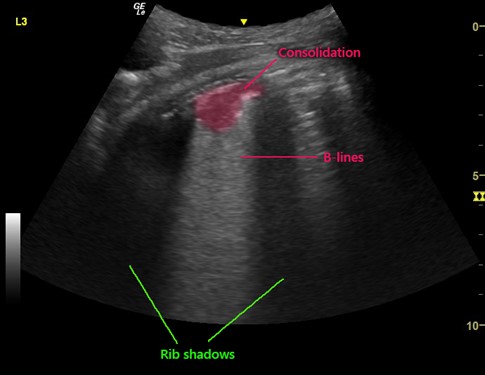
Question: What is seen here and what is the diagnosis? (click to enlarge)
[expand title=”Answer & Explanation:” tag=”h3″]
These videos demonstrate views from the left lateral and posterior thorax. For a review of lung ultrasound zones, see Ultrasound of the Week #014.
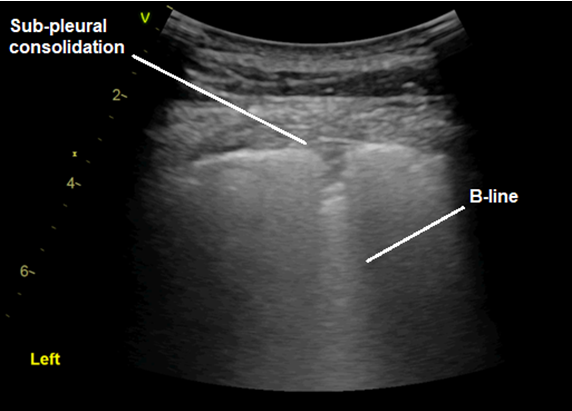
These show pleural irregularity with significant areas of sub-pleural consolidation, from which B lines can be seen emanating, representing alveolar consolidation. There are areas of normal lung nearby.
The distribution of this patient’s consolidation was more upper posterolateral. He was treated with antibiotics, analgesia and oxygen and admitted under the paediatric team.
[expandsub1 title=”Ultrasound in Acute Chest Syndrome:” tag=”h3″]
Acute chest syndrome has a number of causative or contributing factors, including pneumonia (chlamydia, mycoplasma, viral or strep pneumoniae), lung infarction, rib or sternal infarction and fat embolism[1]. Sonographic features include alveolar consolidation, <1cm subpleural consolidations (thought to represent lung infarcts), interstitial syndrome and pleural effusions.
Acute chest syndrome is the leading cause of death of patients with sickle cell disease and so prompt recognition and treatment is essential. Lung ultrasound has been shown to be more sensitive and specific than chest X-ray for the diagnosis of Acute Chest Syndrome[2], and identify abnormalities considerably sooner (3.6 vs. 31.8 hours on average[2]). Patients with SCD and signs of acute chest syndrome will be exposed to a significant amount of ionising radiation over their lifetime, which can be considerably reduced with the adoption of lung ultrasound. This of course requires appropriate governance and documentation of findings.
Review of Lung Ultrasound Technique:
There are a number of protocols for lung ultrasound ‘zones’ when performing a comprehensive examination (see Ultrasound of the Week #014). The general technique involves a ‘lawnmower’ approach using the linear or curvilinear probe, passing horizontally along each rib space before moving down to the below space, ensuring the whole thorax is interrogated. There is an excellent video demonstrating this here at 5 minute sono.
A common pitfall to be aware of is that the sonographic appearances of the liver, spleen, air in the stomach, and thymus can all be easily mistaken for areas of consolidation and hence false positives[3].
[/expandsub1]
[/expand]
[expand title=”References:“]
- Weerakkody, Y., 2021. Sickle cell disease (acute chest syndrome) | Radiology Reference Article | Radiopaedia.org. [online] Radiopaedia.org. Available at: <https://radiopaedia.org/articles/sickle-cell-disease-acute-chest-syndrome-1> [Accessed 9 August 2021]
- Colla JS, Kotini-Shah P, Soppet S, Chen YF, Molokie R, Prajapati P, Prendergast HM. Bedside ultrasound as a predictive tool for acute chest syndrome in sickle cell patients. Am J Emerg Med. 2018 Oct;36(10):1855-1861. doi: 10.1016/j.ajem.2018.07.006. Epub 2018 Jul 3. PMID: 30017686.
- Shah VP, Tunik MG, Tsung JW. Prospective Evaluation of Point-of-Care Ultrasonography for the Diagnosis of Pneumonia in Children and Young Adults. JAMA Pediatrics. 2013;167(2):119. doi:10.1001/2013.jamapediatrics.107
[/expand]