Ultrasound of the Week #041

Case:
A 39 year old male with no PMH presented with 3 days of shortness of breath. That morning he had been unable to get out of bed and called 999. He then collapsed with brief loss of consciousness with paramedics.
Obs on arrival: SpO2 89% on 15L NRBM (0.85 FiO2), RR 34/min, HR 145, BP 120/96
A bedside ultrasound was performed showing the following:
Lung Ultrasound: A-line pattern throughout lung fields with no B-lines, effusions nor consolidation.
Echo:
[expand title=”Findings & Case Progression:” tag=”h2″]
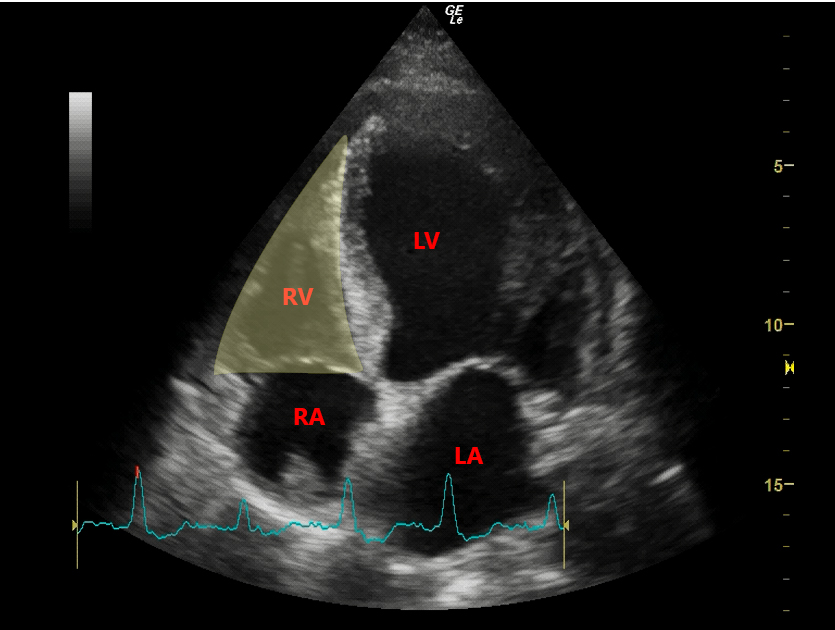
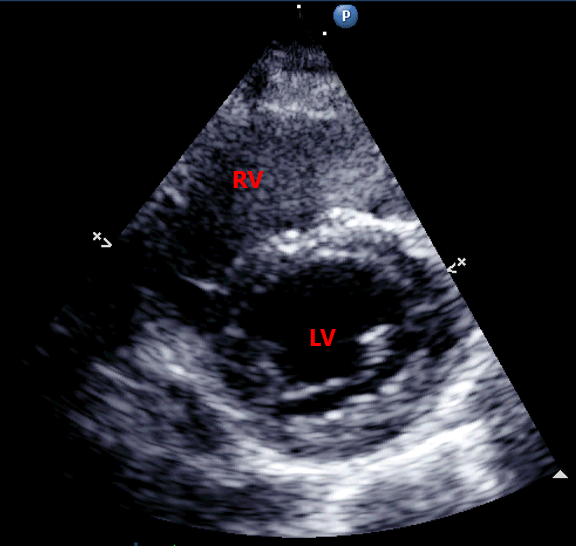
- PSAX: RV:LV ratio >1.0 with interventricular septal flattening (D-sign)
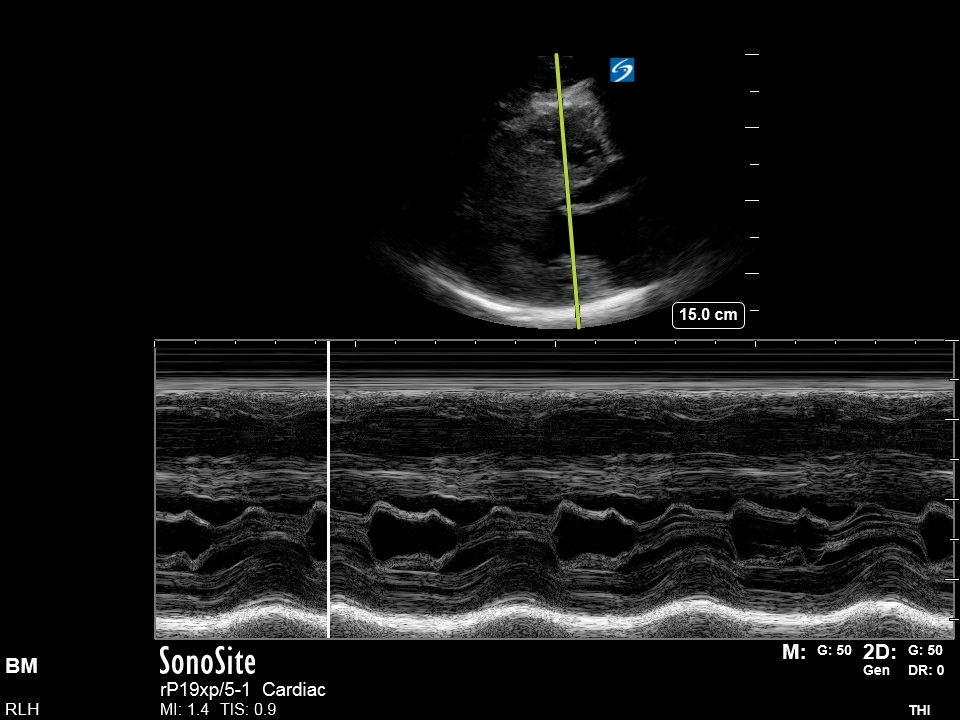
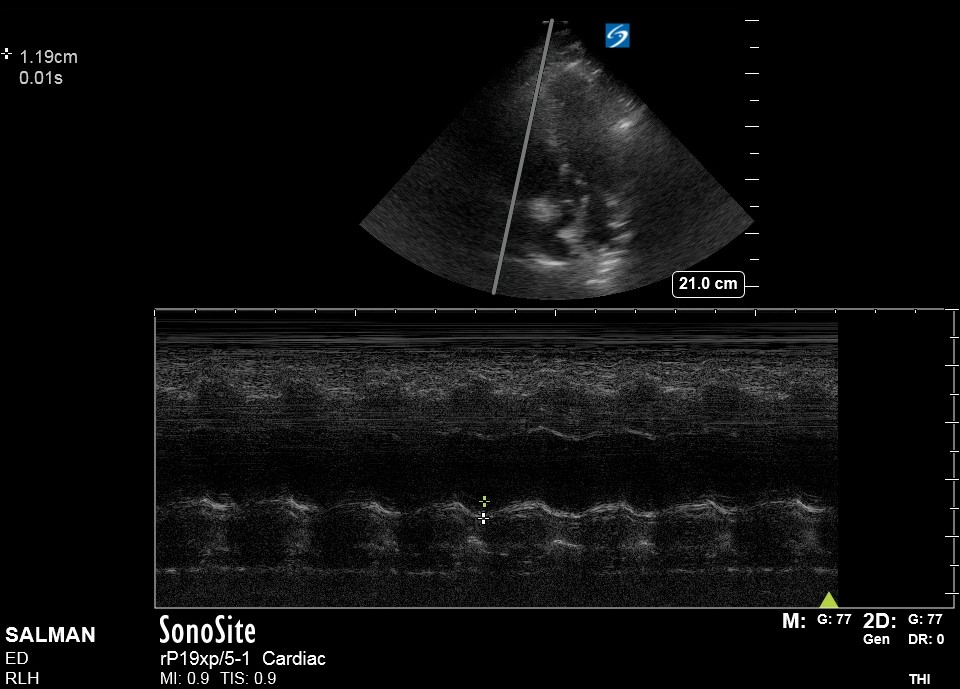
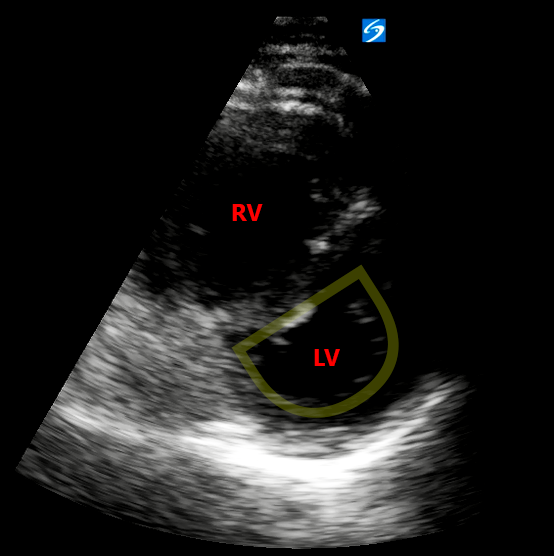
- A4Ch: The LV is notably hyperdynamic with a small LV cavity. The RV is notably dilated with reduced longitudinal function (as indicated by TAPSE) and free wall hypokinesis with apical sparing (McConnell’s sign – see Ultrasound of the Week 039).
- IVC: dilated with no respiratory variation indicating elevated RAP.
Conclusion:
- A-line pattern throughout lung fields
- Hyperdynamic LV with small LV cavity
- RV:LV ratio >1.0 (D-sign)
- Dilated RV with impaired longitudinal function (TAPSE 11.9mm) & McConnell’s sign
- Plethoric IVC
Findings consistent with acute RV failure which along with this history is highly suggestive of acute PE. The lung findings cannot otherwise explain his hypoxia (remember however to always listen for bronchospasm!)
Case Progression:
This is occult shock, with a shock index >1 (HR/SBP), high lactate and an episode of collapse. As such, it was felt he was too unwell for transfer to CT and the decision was made to thrombolyse. He was given 10mg Alteplase over 2 minutes followed by 90mg over 2 hours. He rapidly improved over the next couple of hours, with HR dropping to 108bpm and a massive reduction in oxygen requirement.
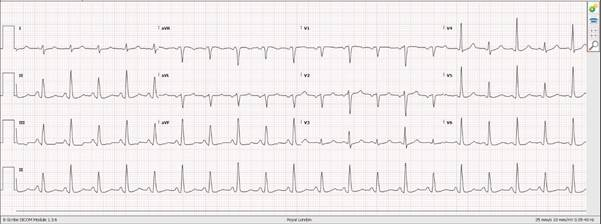
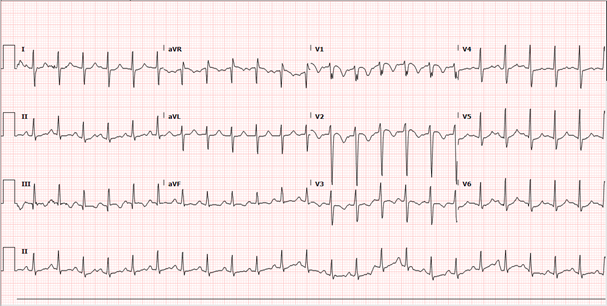
His admission ECG (performed some 30 minutes after POCUS) is shown below with some borderline RAD and RV strain pattern (T wave inversion V1-V3):
He was then sent for CTPA which was reported “Large bilateral pulmonary emboli in left and right pulmonary arteries. Some CT features of right heart strain.“
He was admitted under the acute medical team and the following day (24 hours since POCUS), he had a departmental echo showing a mildly dilated RV with normal systolic function (TAPSE 22mm) and an IVC <2.1cm, varying with respiration. This shows a significant improvement from his POCUS echo and an excellent response to thrombolytics. He remained an inpatient for a few days, improved further and was then discharged with cardiology follow up.
[expandsub1 title=”The Right Heart – an Intro:” tag=”h2″]
The importance of the right heart in cardiac function has been increasingly recognised in recent years and is a fascinating topic, a full description of which is far beyond the scope of this case explanation. In Ultrasound of the Week 039 we discussed McConnell’s sign and sub-massive PEs. Below we go over some basic anatomical features of the RV and how it relates to two POCUS signs of RV-strain – TAPSE and the Eccentricity Index or ‘D-sign’. Details on RV physiology & management of RV failure are not covered here as they are significant topics in themselves. For some truly outstanding explanations of RV failure and management exploring this topic in more depth, I highly recommend the following podcasts and referenced papers, which explain this far better than myself!
- EMCrit 272 – Right Heart Failure with Sara Crager[1]
- Acute Right Heart Failure: Adaptation, Interdependence And External Influences[2]
Anatomy:
Macroscopically, the LV appears bullet-shaped, whereas the adult RV is complex in shape, appearing triangular longitudinally (A4Ch, below) and crescenteric when viewed in cross section (PSAX, below), wrapping or ‘hugging’ around the LV[3,4] (3D image below). This unique shape contributes to differences in RV diastolic & systolic function, as well as adaptations and dysfunction in pathological states.
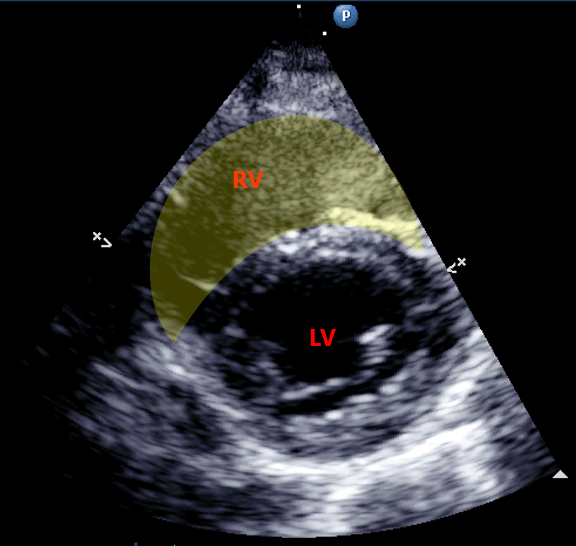
This crescenteric shape in cross section is subject to the position of the interventricular septum (IVS) and distorted in RV volume or pressure overload (as in the D-sign – see below). Since the LV & RV share the same space within the low compliance pericardium, increased filling of one chamber reduces filling of the other. This is known as ventricular interdependence and occurs to a small degree during normal respiration. It is exaggerated in hypovolaemia, RV failure and pericardial tamponade and is the physiological basis behind pulsus paradoxus, stroke volume variation (SVV) and pulse pressure variation (PVV).
Significant acute RV dilation therefore contributes to reduced LV preload and thus SV & CO. This explains the hyperdynamic LV and systemic hypotension seen in massive PE or other forms of acute RV failure.
RV Contraction:
RV contraction occurs via 3 mechanisms[3]:
- Longitudinal base-to-apex contraction, measured by TAPSE (largest contributor to RV systolic output)
- Traction by LV contraction, thickening the IVS and pulling the RV against the LV (20-40% of RV systolic output)
- Inward movement of the RV free-wall in a ‘bellows-like’ effect
Therefore, impaired LV contractility also impairs RV contractility.
[/expandsub1]
[expandsub2 title=”The D-sign or ‘Eccentricity Index’:” tag=”h2″]
The ‘D-sign’ refers to the shape of the LV viewed in PSAX forming a ‘D shape’ rather than its usual round shape, due to rises in RV pressure and dilation cause flattening of the IVS into the LV. This can be measured as the ‘eccentricity index’ which is the LV AP diameter divided by the septal-lateral diameter. A great description of this can be found here at POCUS101[5].
[/expandsub2]
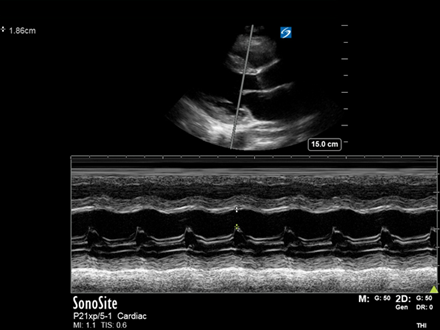
[expandsub3 title=”Tricuspid Annular Plane Systolic Excursion (TAPSE):” tag=”h2″]
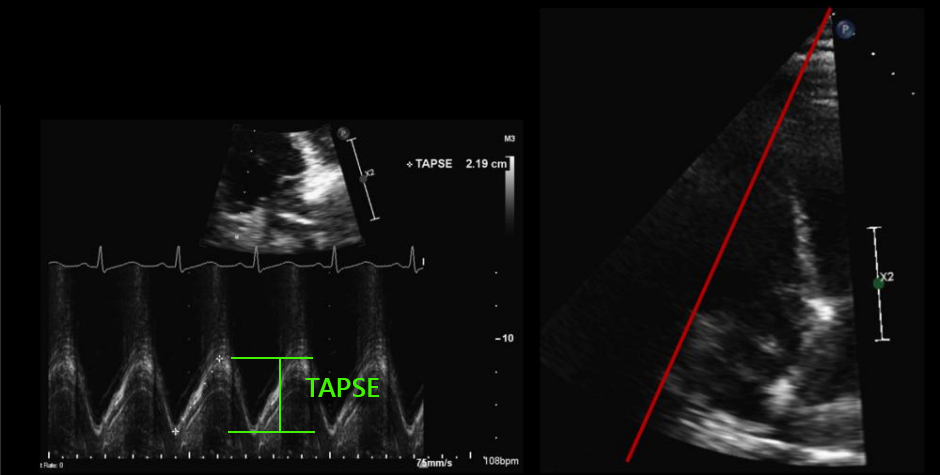
TAPSE measures the base-to-apex contraction of the RV measured in A4Ch using an M-mode cursor through the lateral tricuspid annulus and is the vertical measurement taken from the base (pre-rise) to apex of the trace, a normal TAPSE being ≥17mm.
Since RV myofibrils are mainly arranged longitudinally rather than radially (as LV myofibrils), RV systolic contraction is principally along this axis. TAPSE is therefore an excellent measurement of RV systolic function and prognostic marker in many cardiac conditions including acute PE, with an abnormal TAPSE independently correlated with increased short-term mortality[6,7,8] and ICU length of stay.
Note: It is important the M-mode cursor is aligned parallel with the tricuspid annular movement in order to avoid underestimation.
[/expandsub3]
[expandsub4 title=”Summary & Learning Points:” tag=”h2″]
- In an acutely unwell patient with a high pre-test probability of pulmonary embolism, focused lung and cardiac ultrasound can provide supporting evidence for early thrombolysis
- The RV is paramount in maintaining normal CO and RV dysfunction carries a poor prognosis
- The Eccentricity Index or ‘D-sign’ can be used to assess RV volume or pressure overload
- TAPSE measures RV longitudinal function and is an important prognostic indicator in RVF
- RV failure is considered the ‘common final pathway’ in CCF as well as other conditions and carries a high mortality[9]
[/expandsub4]
[/expand]
[expand title=”References:“]
- Scott Weingart, MD FCCM. EMCrit 272 – Right Heart Failure with Sara Crager. EMCrit Blog. Published on April 29, 2020. Accessed on July 31st 2021. Available at [https://emcrit.org/emcrit/right-heart-sara-crager/ ].
- Michael Pinsky Acute right heart failure: Adaptation, interdependence and external influences by Professor Michael Pinsky, CICM 2018 Annual Scientific Meeting
- Sheehan F, Redington A, The right ventricle: anatomy, physiology and clinical imaging Heart2008;94:1510-1515.
- Anavekar NS, Gerson D, Skali H, Kwong RY, Yucel EK, Solomon SD. Two-dimensional assessment of right ventricular function: an echocardiographic-MRI correlative study. Echocardiography. 2007 May;24(5):452-6. doi: 10.1111/j.1540-8175.2007.00424.x. PMID: 17456062.
- Dinh, V., 2021. The D Sign – Right Heart Strain from Pressure vs Volume Overload – POCUS 101. [online] POCUS 101. Available at: <https://www.pocus101.com/the-d-sign-right-heart-strain-from-pressure-vs-volume-overload/> [Accessed 31 July 2021].
- Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. 2008 Mar 18;117(11):1436-48. doi: 10.1161/CIRCULATIONAHA.107.653576. PMID: 18347220.
- Lobo, J.L., et al., Prognostic significance of tricuspid annular displacement in normotensive patients with acute symptomatic pulmonary embolism.J Thromb Haemost, 2014. 12(7): p. 1020-7.
- Giovanardi P, Tincani E, Maioli M, Tondi S. The Prognostic Importance of TAPSE in Early and in Stable Cardiovascular Diseases. J Cardiovasc Dev Dis. 2020 Jan 15;7(1):4. doi: 10.3390/jcdd7010004. PMID: 31952140; PMCID: PMC7151306.
- Voelkl N. F., Quaife R. A., Leinwand L. A., Barst R. J., McGoon M. D., Meldrum D. R., Dupuis J., Long C. S., Rubin L. J., Smart F. W., Suzuki Y. J., Gladwin M., Denholm E. M., & Gail D. B. National Heart, Lung, and Blood Institute Working Group on Cellular and Molecular Mechanisms of Right Heart Failure. Right ventricular function and failure. Report of the National Heart, Lung, and Blood Institute working group on cellular and molecular mechanisms of right heart failure. Circulation. 2006 Oct. 24 114 (17): 1883-91.
[/expand]