Ultrasound of the Week #030
Case:
A 16 year old male presented with significant abdominal pain and some chest discomfort requiring morphine.
BP was 97/48, HR 108bpm, SpO2 98% on room air.
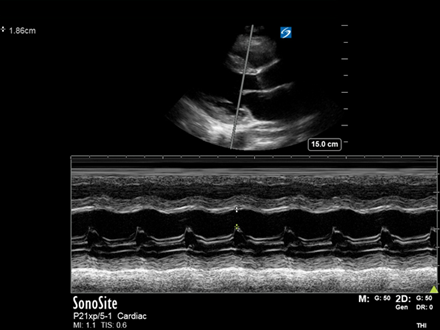
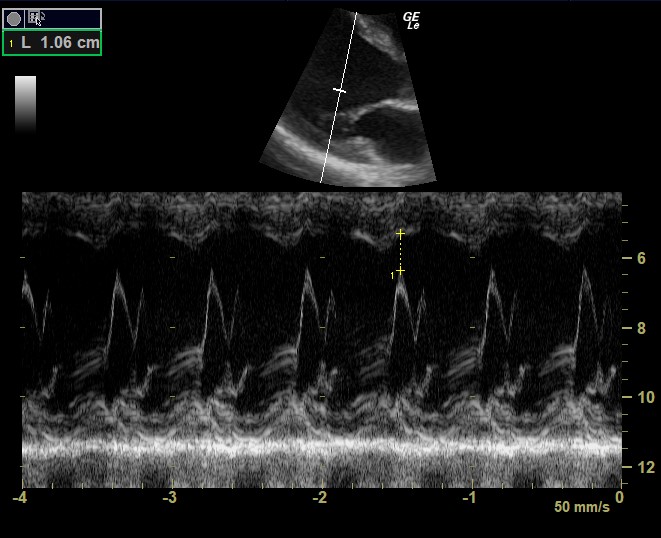
He had a bedside echo – see attached videos and pics below.
Question: What does the echo show?

There is notably impaired LV systolic function, with no obvious RWMA. The EPSS (E-point Septal Separation) is 10.6mm (with >7mm indicating impaired LVEF). The TAPSE is 19.1mm (>16mm reflecting normal RV longitudinal function). There is no obvious chamber dilation and there were no significant valvular abnormalities noted. There is a very small pericardial effusion visible in the subcostal view and a small right sided pleural effusion.
Blood tests revealed CRP 204, Trop 238 and BNP 4619. He was admitted under paediatrics and seen by the ID team, treated for likely PIMS-TS. He received cautious fluid boluses for his hypotension and was started on methylprednisolone, aspirin, LMWH, antibiotics and later received treatment with IVIG. He remained intermittently hypotensive yet improved during his stay and was discharged some days later, for a follow up echocardiogram 6 weeks post-discharge.
For a review of EPSS, see Ultrasound of the Week #006, and TAPSE in Ultrasound of the Week #009.
[/expand]