Ultrasound of the Week #047

Case:
A 64 year old male with PMH only of AF was sent to the Emergency Department from stroke rehabilitation with lethargy, confusion and feeling generally unwell.
Haemodynamically he was within normal limits, BP112/76. Chest clear. Abdomen was soft with palpable hepatomegaly.
Blood gas showed pH 7.36, pCO2 2.3, BE-9, lactate 6 and Cr 180, K+ 5.4. Hb 128. ALT 894, Bili 24.
The EM SpR was asked to perform an US aorta to rule out AAA showing the below:

[expand title=”Answers & Explanation:” tag=”h2″]
[expandsub1 title=”POCUS Findings:” tag=”h2″]
Findings:
- No AAA
- Intraperitoneal free fluid
- LV: non-dilated, good contractility
- RV: dilated, impaired longitudinal function. Septal flattening
- MV: echogenic mobile mass, significant MR
- IVC: plethoric
Conclusion:
- Adequate LV preload and contractility.
- High RV preload with impaired systolic function and echo signs of RV strain
- MR with mobile MV mass
- Plethoric IVC indicating elevated right sided filling pressures
- Significant intraperitoneal free fluid with no AAA and dilated intraperitoneal veins.
These findings are consistent with RV failure in the context of significant MR. His blood tests and clinical picture suggest congestive hepatic and renal failure secondary to RV failure – ‘cardiorenal syndrome’. An explanation of this congestion is given below.
[/expandsub1]
[expandsub2 title=”Case Progression:” tag=”h2″]
The patient received diuresis and was admitted under the medical team (despite discussion around diuresis vs fluids for hypotension – more below!). A departmental echo confirmed severe MR due to papillary muscle rupture (the echogenic mass). The following day he deteriorated on the ward, requiring a peri-arrest call, admission to ICU where he was supported on noradrenaline and milrinone prior to a critical transfer for emergency mitral valve repair.
Blood Pressure, Perfusion & Flow:
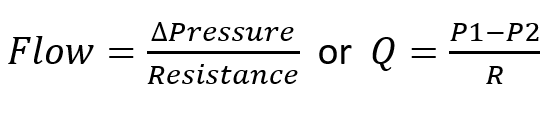
A major determinant of organ perfusion is blood flow. Blood flow through an organ is determined by pressure difference and resistance.
Maximal organ perfusion pressure is MAP – CVP and therefore as CVP rises, organ perfusion drops. This is the physiological basis behind organ congestion and dysfunction in RV failure and elevations in CVP are associated with increased mortality and AKI[3,4]. BP is not the sole determinant of organ perfusion.
[/expandsub2]
[expandsub3 title=”Right Heart Failure:” tag=”h2″]
Disclaimer – this is a massive topic! The right heart is complex and we previously reviewed some aspects of this in Ultrasound of the Week 039 & 041. Below is briefly discussed the physiology of flow & congestion, RV perfusion and pulmonary vascular resistance (PVR). Again, for some truly outstanding explanations of RV failure and management exploring this topic in more depth, I highly recommend the following podcasts and referenced papers, which explain this far better than myself!
- EMCrit 272 – Right Heart Failure with Sara Crager[1]
- Acute Right Heart Failure: Adaptation, Interdependence And External Influences[2]
The bottom line – RV failure is complex and if you’re not sure – don’t give fluids! Ask for help!
This week we briefly discuss RV perfusion, RV afterload and the importance of maintain a good systemic blood pressure.
RV:PVR Relationship and Cardiac Output:
RV failure can occur through 2 principle mechanisms : elevated RV afterload (e.g PE, LVF, COPD) or myocardial failure (e.g. MI/myocarditis). The most common cause of RV failure is LV failure.
After birth, following a dramatic reduction in pulmonary vascular resistance (PVR), the RV changes from a high pressure system to a low pressure system, with its thinner myocardium reflecting this. As such, the RV cannot produce elevated pressures (unlike the LV) and so to increase cardiac output, PVR must drop. This occurs through recruitment and distension of the pulmonary vasculature[5]. For the RV we can therefore write:

mPAP = mean Pulmonary Arterial Pressure, PAOP = Pulmonary Artery Occlusion Pressure (surrogate for LAP)
This explains why the RV struggles with rapid elevations in PVR (e.g. in massive PE). If PVR cannot be reduced (as in PE or untreated pulmonary hypertension), CO will drop once maximal RV pressures have been reached (usually 20-30mmHg). Chronic elevations in PVR will lead to adaptive RV hypertrophy and as such these hearts are able to generate higher RV pressures.
Tip: a hypertrophied RV (free wall in diastole >5mm) suggests chronic pulmonary hypertension.
PVR is further increased by the following:
- Hypoxia – pulmonary hypoxic vasoconstriction
- Hypercapnia
- Acidosis
- Excessively high or low lung volumes – PVR is lowest at FRC
- Elevated alveolar pressures – avoid positive-pressure ventilation.
Reducing PVR can be attempted through targeting the above, or through IV/inhaled pulmonary vasodilators (e.g Nitric Oxide, esoprostenol).
RV Perfusion:
RV perfusion occurs predominantly via the right coronary artery (RCA), with a perfusion pressure gradient determined by (aortic – RV intracavitary pressure). In contrast to the LV, RV perfusion therefore occurs during both diastole & systole in healthy individuals, since a normal RV pressure is roughly 15-30mmHg (systole) and 0-10mmHg (diastole), considerably less than the 120/80mmHg in the aorta.
A rise in RV intracavitary pressure (e.g. pulmonary hypertension) or drop in SBP will therefore reduce RCA systolic flow and perfusion becomes predominantly diastolic, leading to RV ischaemia. Optimising RV perfusion therefore requires maintaining systemic blood pressure (↑SVR) whilst minimising rises in RV afterload (↓PVR).
The Failing RV:
For any given PVR, if RV contractility is impaired, SV can only be maintained by RV dilation. If this happens acutely, RV wall stress increases and RV perfusion is impaired. Additionally, LV filling is impaired through ventricular interdependence and MAP falls, further impairing RV perfusion. RV ischaemia then leads to wall stiffness and reduced contractility and the situation spirals, ultimately leading to cardiovascular collapse and cardiac arrest.

[/expandsub3]
[expandsub4 title=”Management principles of RV failure:” tag=”h2″]
- High HR & sinus rhythm to prevent RV distension and maintain CO.
- Optimise preload – diuresis if overfilled, cautious fluid if underfilled.
- Maintain perfusion – increase SVR
- Maintain contractility – inotropes e.g. milrinone, dobutamine, levosimendan
- Reduce RV afterload – decrease PVR. Avoid intubation as much as possible.
[/expandsub4]
[expandsub5 title=”Summary & Learning Points:” tag=”h2″]
- Organ perfusion is dependent on MAP and CVP
- RV failure causes systemic organ congestion. Do not fluid resuscitate cor pulmonale.
- RV perfusion occurs during both systole & diastole and it is very prone to ischaemia
- The RV cannot handle significantly elevated afterload (PVR).
- The failing RV can spiral leading to rapid multi-organ failure and death.
[/expandsub5]
[/expand]
[expand title=”References:“]
- Scott Weingart, MD FCCM. EMCrit 272 – Right Heart Failure with Sara Crager. EMCrit Blog. Published on April 29, 2020. Accessed on July 31st 2021. Available at [https://emcrit.org/emcrit/right-heart-sara-crager/ ].
- Michael Pinsky Acute right heart failure: Adaptation, interdependence and external influences by Professor Michael Pinsky, CICM 2018 Annual Scientific Meeting
- Chen CY, Zhou Y, Wang P, Qi EY, Gu WJ. Elevated central venous pressure is associated with increased mortality and acute kidney injury in critically ill patients: a meta-analysis. Crit Care. 2020 Mar 5;24(1):80. doi: 10.1186/s13054-020-2770-5. PMID: 32138764; PMCID: PMC7059303.
- Wang X, Chen H, Liu D, Zhang Q, Su L. The correlation between CVP-derived parameters and the prognosis of critically ill patients. J Crit Care. 2017 Aug;40:257-264. doi: 10.1016/j.jcrc.2017.03.011. Epub 2017 Mar 16. PMID: 28666246.
- John B. West, Andrew M. Luks, West’s Respiratory Physiology: The Essentials, Seventh Edition. Wolters Kluwer, 2016
- Voelkl N. F., Quaife R. A., Leinwand L. A., Barst R. J., McGoon M. D., Meldrum D. R., Dupuis J., Long C. S., Rubin L. J., Smart F. W., Suzuki Y. J., Gladwin M., Denholm E. M., & Gail D. B. National Heart, Lung, and Blood Institute Working Group on Cellular and Molecular Mechanisms of Right Heart Failure. Right ventricular function and failure. Report of the National Heart, Lung, and Blood Institute working group on cellular and molecular mechanisms of right heart failure. Circulation. 2006 Oct. 24 114 (17): 1883-91.
[/expand]