Ultrasound of the Week #023

A little more paeds this week. Special thanks to Dr Dominic Craver, PEM Senior Clinical Fellow for this great case.
Case:
An 8 week old female baby was brought to ED after Mum noticed when changing nappy that her left leg was being held in flexion at the hip and seemed uncomfortable.
She had a PMH of Group B strep left hip septic arthritis diagnosed at day 7 of life which required wash out and 6 weeks IV antibiotics which she had completed and her PICC had been removed 7 days prior to attendance. She had been well since discharge and had been moving left hip normally
Pregnancy history:
Born 40/40 by normal vaginal delivery with no perinatal complications
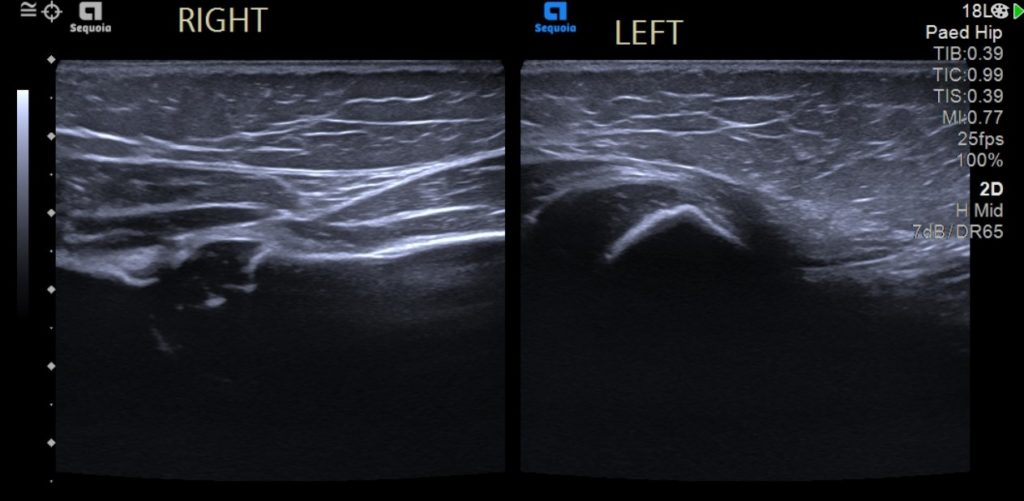
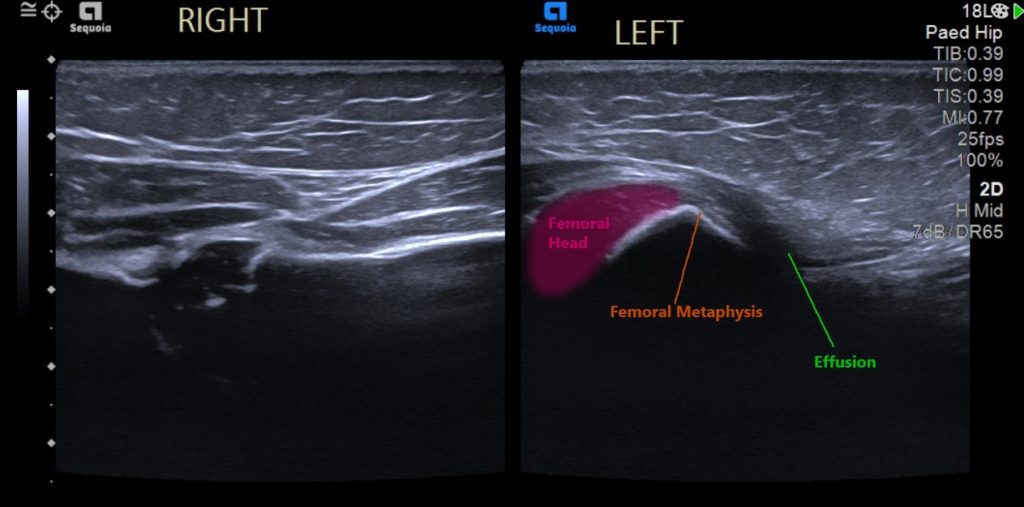
A bedside POCUS of her hips was performed by the PEM SpR with the following images:
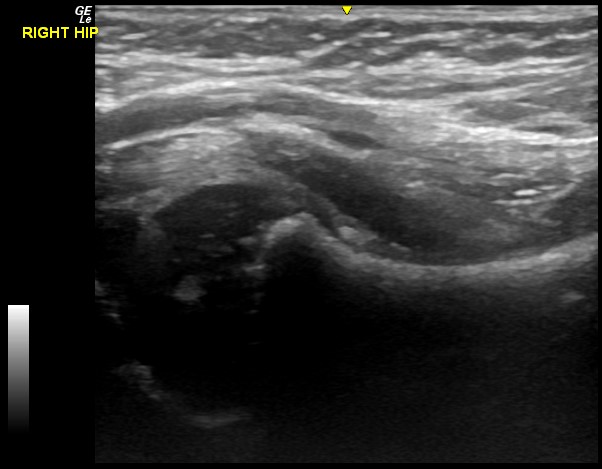
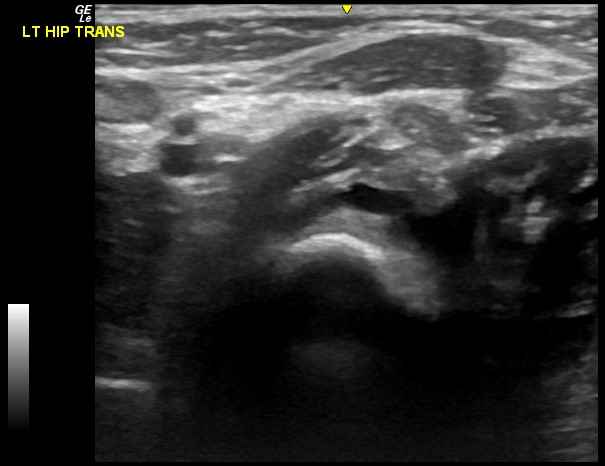
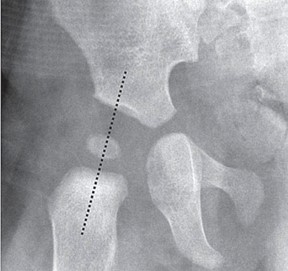
Sadly as the SpR was working alone, a longitudinal view of the left hip (demonstrating the effusion better) was not captured, but an effusion can be seen in the transverse view. Below are the longitudinal radiology images which demonstrate the two side by side nicely:
Here you can see where the effusion is identified.
The patient was admitted under the paediatric surgical team for further assessment.
[expand title=”POCUS for hip effusions in Paediatrics:” tag=”h2″]
With a small amount of training, PEM physicians can accurately identify hip effusions with a high degree of sensitivity and specificity.[1] Whilst this cannot distinguish transient synovitis of the hip from septic arthritis, the absence of an effusion can confidently exclude the diagnosis.
The sonographic criteria for a paediatric hip effusion are:[2]
- Synovial Fluid collection greater than 5mm OR
- >2mm difference when compared to the asymptomatic contralateral hip
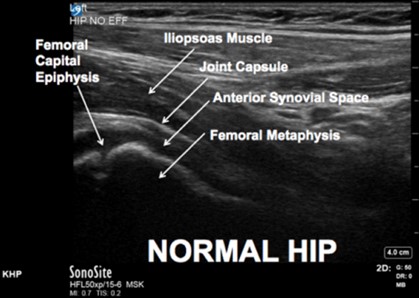
The anterior approach is ideal to assess the presence of joint fluid in a child of any age. The hip joint is examined with the high frequency transducer positioned obliquely along the long axis of the femoral neck as shown below.
Images courtesy of ACEP, available at https://www.acep.org/how-we-serve/sections/emergency-ultrasound/news/april-2018/tips–tricks-ultrasound-in-the-diagnosis-of-a-pediatric-hip-effusion/
Both hip joints should be imaged for comparison. The patient is positioned in a neutral position with the legs straight and the feet slightly externally rotated.
If pain prohibits a neutral position, the contralateral leg should be positioned in a mirror image to the affected side, thus allowing a true comparison of anatomy and pathology.
The ultrasound image should include the joint space, head of femur, neck of femur, joint capsule and overlying iliopsoas muscle. The normal joint capsule follows the contour of the neck of femur in a concave shape. The normal anterior and posterior joint capsule layers abut each other. When an effusion is present, the two layers of joint capsule are separated by fluid, causing the anterior layer to become convex in relation to the neck of the femur. An infective process may also display hyperaemia of the tissues around the area of infection evident on colour Doppler.
Other pathologies that may be diagnosed with ultrasound in a limping child include SUFE, avascular necrosis, tumours, and fractures such as toddler’s fracture.
[/expand]References: