Ultrasound of the Week #036

Case 1:
A 14 year old male was brought in as a trauma call having fallen from a scooter. His left leg was in a Kendrick splint having had notable deformity on scene. Primary survey confirmed the left thigh pain and deformity and XR showed the following:
No other injuries were identified and he was admitted to a paediatric bed under the trauma team. Ketamine sedation was planned in order to put his left leg into traction but as an alternative, a femoral nerve block (FNB) was offered.
This was performed under ultrasound guidance in resus and 13ml of 0.25% bupivacaine (2.5mg/ml = 32.5mg) was infiltrated around the femoral nerve with no immediate complications.
20 minutes later the patient had his Kendrick splint removed, was put into skin traction and transferred to a hospital bed whilst using his phone and reporting no pain throughout. He was then transferred to the ward and had effective ongoing anaesthesia overnight. He was very happy with his pain relief and was glad that he chose to go ahead with a nerve block.
Case 2:
A 2 year old male with known talipes was brought in in the early hours having slipped in his talipe-correction boots and twisted his left leg. The left thigh was notably swollen and he was in considerable pain, unwilling to move from sitting nor have his left leg touched. He also had a PMH of enlarged adenoids and tonsils, with stridor at rest for which he was awaiting surgery.
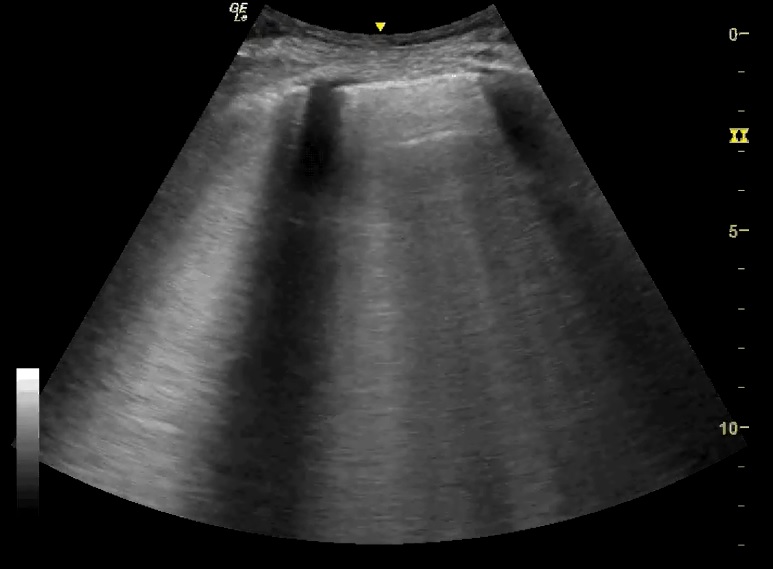
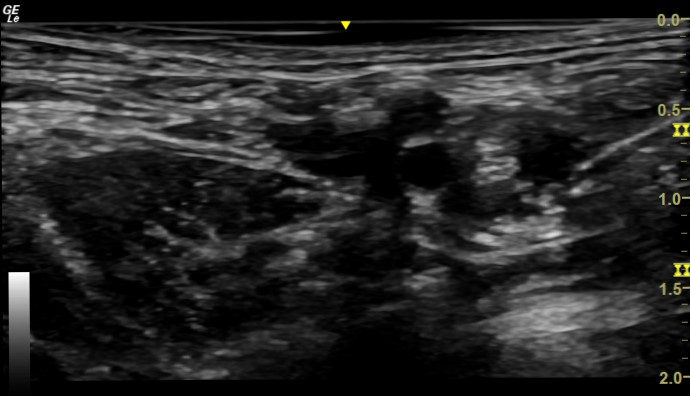
He received paracetamol and ibuprofen at triage. A gentle ultrasound of his left thigh showed the following:
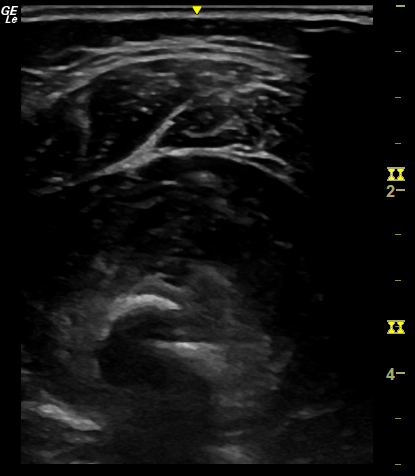
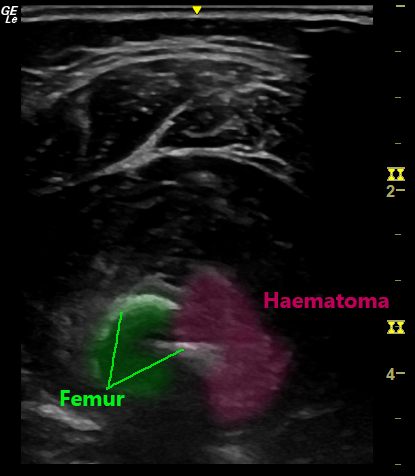
This demonstrates a break in the cortex of the femur with surrounding haematoma, confirming the suspected femoral shaft fracture.
Given his adenoid/tonsillar enlargement, it was felt that sedation overnight would not be appropriate and so LMX gel was placed in his left femoral crease in preparation for a nerve block. This was performed 40 minutes later after some intranasal fentanyl, using 4.5ml 0.25% bupivacaine (images below).
15 minutes later the child was happy and comfortable transferring to XR and having his leg manipulated for imaging. This was then later placed in skin traction and he was listed for theatre the following day.


The use of US in these cases allowed for effective analgesia for procedures & diagnostics in ED and many hours afterwards, avoiding need for sedation and side effects of systemic analgesics. In Case 2 US facilitated diagnosis and nerve block prior to imaging, significantly improving patient comfort throughout their ED stay.
Ultrasound Guided Femoral Nerve Block:
Femoral Nerve Block (FNB) has long been a technique used for anaesthesia of femur fractures. Ultrasound-guided blocks have been shown to be faster and more efficacious than nerve-stimulator guided blocks[1,2] and are relatively simple to perform.
Below is a brief description of the technique, but there is an excellent summary by NYSORA here[3].
The patient should be monitored and sterility observed throughout the procedure.
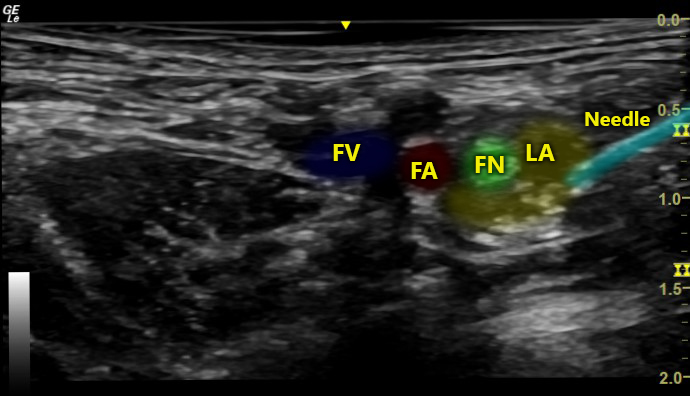
With the linear (high-frequency) ultrasound probe positioned transversely in the femoral crease, the femoral nerve is located lateral to the femoral artery. Tip: tilting the transducer cranially or caudally can help improve visualisation of the femoral nerve.
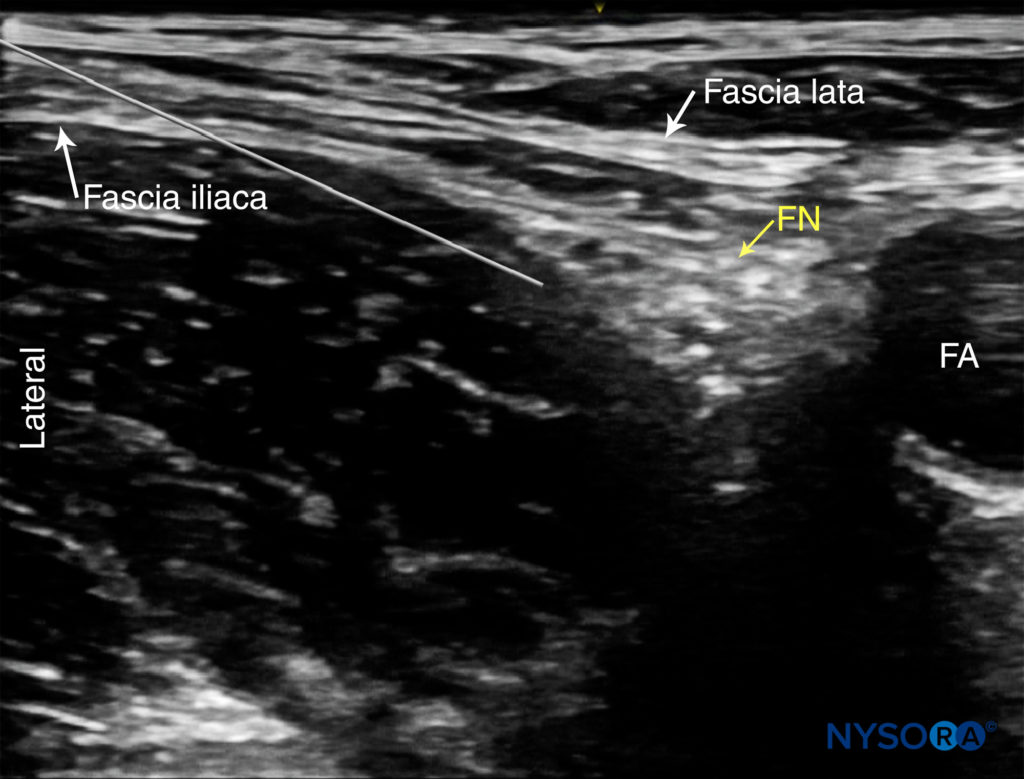
After anaesthetising the skin with lidocaine, a short-bevel, 20-22G needle is advanced in-line with the transducer from lateral to medial under direct visualisation. Passage through the fascia iliaca should be felt and the tip of the needle positioned just lateral to the femoral nerve.
An assistant then aspirates (ensuring no blood aspirate) and injects a small amount of local anaesthetic under direct US visualisation. There should be little resistance to injection. High resistance suggests intrafascicular or incorrect fascial plane position of the needle tip.
LA should displace the femoral nerve medially, away from the needle, or should disperse above/below the femoral nerve. 10-15ml of LA is required in an adult.
Femoral Nerve Block vs Fascia Iliaca Block:
A few trials have compared FNB vs Fascia Iliaca Block (FIB) vs ‘3-in-1’ Block[1,4]. There is little convincing evidence to suggest that either of the three is superior, and that pain scores do not vary significantly between the different blocks.
There is a theoretically (albeit unproven) higher risk of vascular or nerve injury with FNB, although with US guidance this should not be significant with an experienced operator.
One advantage of FNB is that it requires a smaller volume of local anaesthetic and so should be considered if LA is required at other sites.
US-guided FIB will be added to the new RCEM Ultrasound Curriculum as of August 2021. The skills required and technique are easily transferable between FNB/FIB and many other nerve blocks, and familiarisation with ‘needling’ under US guidance is extremely useful for EM physicians. Early effective analgesia is a fundamental part of good Emergency Care and regional blocks are an excellent way to provide this.
References:
- Newman B, McCarthy L, Thomas PW, May P, Layzell M, Horn K. A comparison of pre-operative nerve stimulator-guided femoral nerve block and fascia iliaca compartment block in patients with a femoral neck fracture. 2013; 68(9):899-903. PMID: 23789738
- Forouzan A, Masoumi K, Motamed H, Gousheh MR, Rohani A. Nerve Stimulator versus Ultrasound-Guided Femoral Nerve Block; a Randomized Clinical Trial. Emergency (Tehran, Iran). 2017 ;5(1):e54.
- Atchabahian, A., Leunen, I. and Vandepitte, C., 2021. Ultrasound-Guided Femoral Nerve Block – NYSORA. [online] NYSORA. Available at: https://www.nysora.com/techniques/lower-extremity/ultrasound-guided-femoral-nerve-block [Accessed 9 June 2021].
- Reavley P, Montgomery AA, Smith JE, et al. Randomised trial of the fascia iliaca block versus the ‘3-in-1’ block for femoral neck fractures in the emergency department.Emerg Med J. 2015; 32(9):685-689