Ultrasound of the Week #038
Case:
A 4 year old male presented with generalised abdominal pain and vomiting. He had had on & off abdominal pain since an open appendicectomy 3 months previously, but this had worsened in the last 24 hours.
He had eaten and passed stool that morning.
A bedside ultrasound of his abdomen was performed in ED.
Question: What does this show?
[expand title=”Answer: ” tag=”h2″]
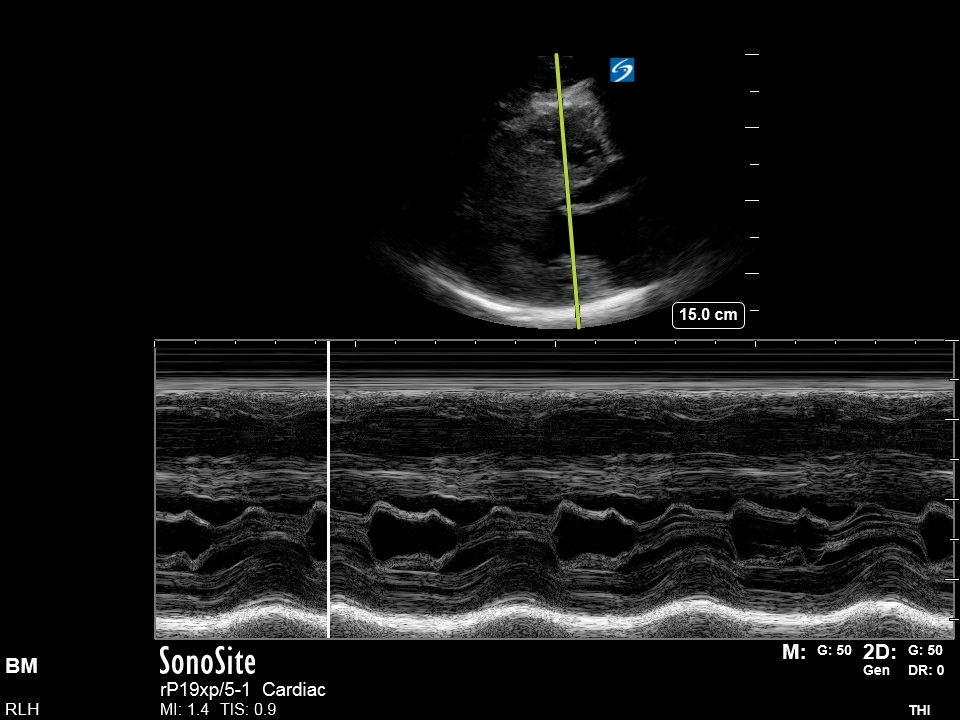
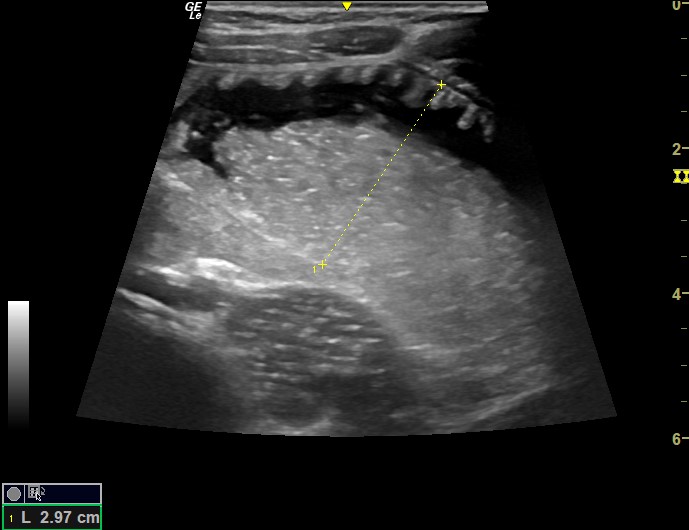
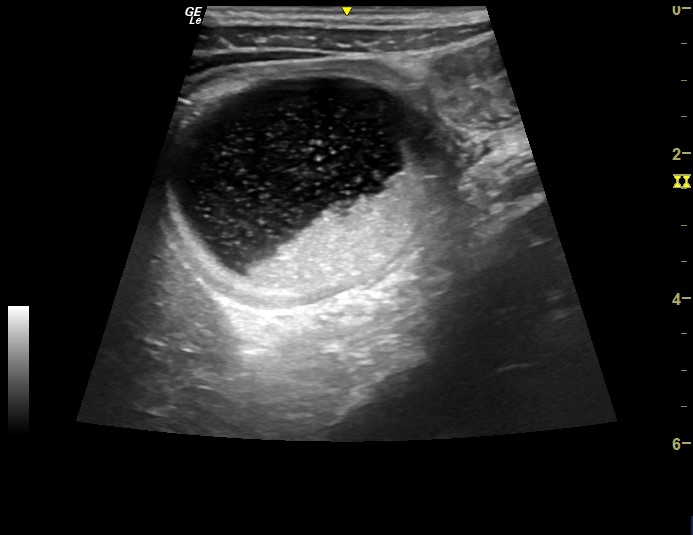
Dilated loops of small bowel are seen, with anterograde and retrograde movement of bowel contents within. Abdominal free fluid can also be seen outside the loops of bowel. This is small bowel obstruction.
He was admitted under surgeons and had a trial of conservative management with NG tube and IV fluids, and unfortunately had to have a laparotomy and adhesiolysis 2 days later. He was discharged 4 days later.
[expandsub1 title=”Evaluation for Small Bowel Obstruction (SBO) with POCUS: “]
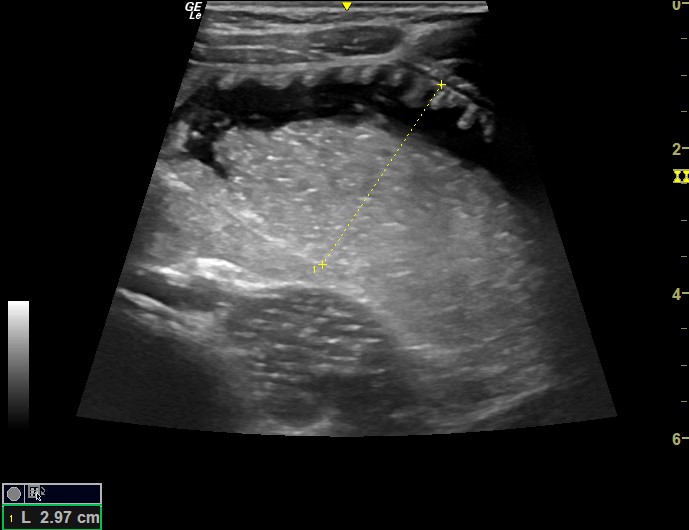
Small bowel obstruction can be readily identified using bedside ultrasound. Classic findings in SBO include dilated loops of fluid-filled bowel (>2.5cm) and anterograde & retrograde (back & forth) movement of intraluminal contents.
Small bowel can be recognised by the valvulae conniventes which become evident when surrounded by fluid and this is often referred to as the ‘keyboard sign’.
A number of studies have demonstrated the superiority of US over AXR for the diagnosis of SBO, with systematic reviews and meta-analyses demonstrating that in patients with a clinical suspicion of SBO, ultrasound outperformed AXR and even MRI/CT[1,2]. POCUS is cheap, radiation free, available in resource-stretched environments and dynamic, allowing real-time visualisation of intraluminal content movement. Furthermore, it is easy to learn given an appropriate teaching process – a 2010 study by Tang et al demonstrated that following only a 10-minute teaching session and 5 US scans for SBO, Emergency Physicians using POCUS significantly outperformed AXRs reported by Consultant Radiologists in diagnosing SBO[3].
There is an excellent article with more information on US assessment of SBO by ACEP here[4].
[/expandsub1]
[/expand]
References: