Ultrasound of the Week #048

Case:
A 68 year old patient who was recently discharged from hospital after being treated for complicated UTI presented with 3 days of swelling of the abdomen with inability to pass urine. On initial examination he was frail with a distended, soft abdomen. Given the extent of distension it was decided to do an extended examination of the abdomen with ultrasound.
Findings:
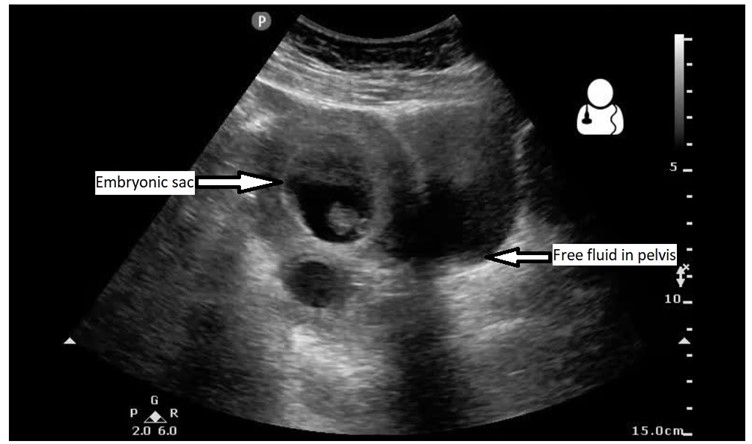
RUQ window showed the following:
The above image shows right kidney with multiple hypoechoic (dark) cavities in the cortex with some hyperechoic debris inside. One of the differentials is renal abscess. There is also a rim of black line in between the kidney the liver which shows free fluid in the peritoneum.
LUQ window:
Again this shows multiple hypoechoic cavities in the cortex of the left kidney.
Suprapubic view:
This is an excellent view which helped us diagnose why the patient’s catheter was not draining after being changed in the department. It shows a distended urinary bladder with a lot of hyperechoic debris and the bulb of the urinary catheter in the middle.
PoCUS is an excellent modality to troubleshoot catheter problems i.e misplacement, blockage.
US is an initial investigation of choice for kidney masses and cysts. It helps to differentiate between simple and complex cysts, although CT is the gold standard. In a sick patient where CT is not possible PoCUS can help to find out the cause of AKI and guide treatment.
Further scanning of the umbilical region was done which showed:
This view shows dilated small bowel loops with heterogenous fluid in the lumen. You can also visualise the valvulae conniventes in the left side of the window.
Ultrasound of the small bowel:
Ultrasound has a very high accuracy of diagnosing small bowel obstruction, although is limited in reporting the site of obstruction and the cause. Dilated bowel on US had a sensitivity of 91% (95% CI 75 to 98%) and specificity of 84% (95% CI 69 to 93%) for SBO, compared to 27% (95% CI 14 to 46%) and 98% (95% CI 86 to 100%) for decreased bowel peristalsis on US. X-ray had a sensitivity of 46.2% (95% CI 20.4 to 73.9%) and specificity of 66.7% (95% CI 48.9 to 80.9%) for SBO when diagnostic, but was non-diagnostic 36% of the time.[1]
Criteria for diagnosis of SBO:
A positive ultrasound was defined as either:
- Dilated loops (>2.5cm) of fluid-filled dilated bowel proximal to normal/collapsed bowel
- Presence of the keyboard sign
- Reduced peristalsis – back-and-forth movement of spot echoes inside fluid-filled bowel ( see video attached )
Case progression:
This allowed us to put in NG tube to decompress the small bowel and catheter was flushed multiple times and it got blocked multiple times.
CT AP was requested however radiology initially refused to do. POCUS findings helped us to push our case and finally they agreed and CT confirmed small bowel obstruction with bilateral multiple renal abscesses and a psoas abscess.
Benefit of bedside sonography:
This case highlights the use of extended examination with US in a sick patient. Bedside US allowed us to diagnose the patient at bedside, instigate treatment, expedite specialist input, monitor the patient and push for confirmatory radiological investigation.
References: