Ultrasound of the Week #015
A paediatric case this week! Ultrasound in paediatrics is becoming increasingly used due to it’s safety profile, ease of use and generally high diagnostic accuracy.
Special thanks to Dr Mahmoodian for this interesting case and images.
Case:
A 3 year old male attended ED with intermittent abdominal pain and fever. He had attended UTC 2 days prior and been discharged as possible GORD/constipation with Gaviscon.
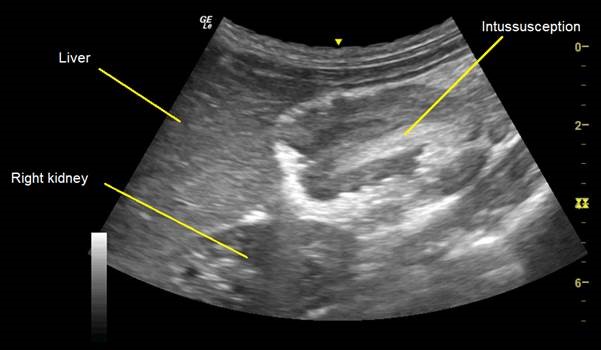
He had a bedside ultrasound showing the following:
Question: What do these images show?
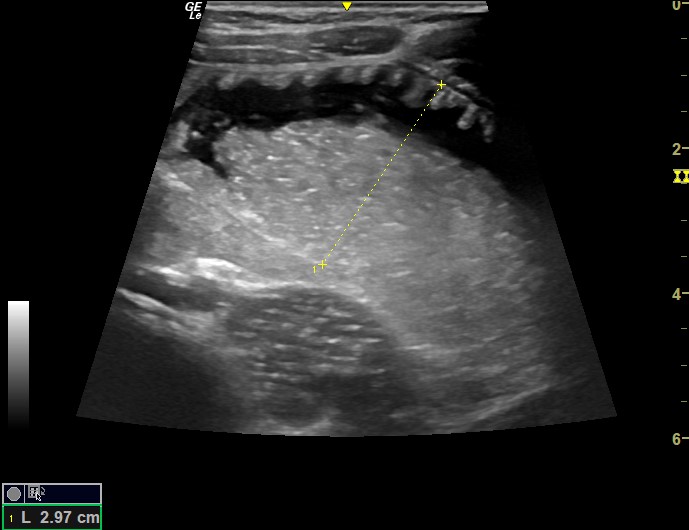
[expand title=”Interpretation” tag=”h2″]This is intussusception. Viewing in transverse cross-section shows the classic ‘target’, ‘bulls eye’ or ‘doughnut’ sign (seen below). This target is usually ≥3 cm in diameter. There is also a small amount of free fluid visible in this case:
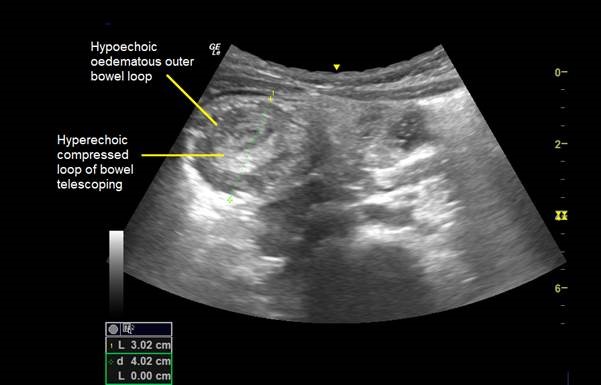
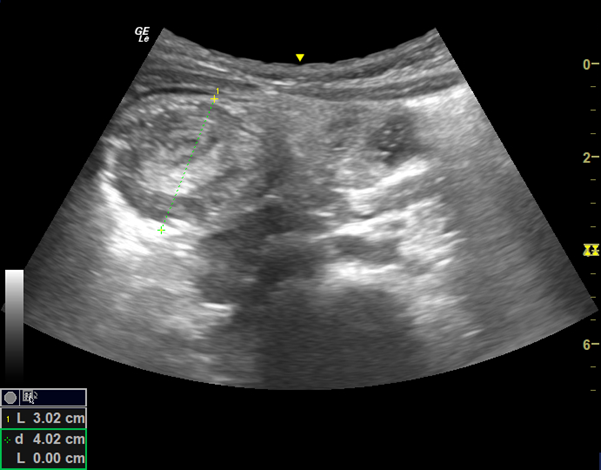
Viewing the intussusception in longitudinal view shows the ‘pseudokidney’ or ‘sandwich’ sign (seen below). The intussusception can appear like a kidney as the mesentery and associated vessels appear similar to the renal hilum:
[expandsub1 title=”POCUS for Intussusception:“]
Bedside ultrasound for intussusception may lead to more expeditious diagnosis particularly when paediatric radiology is not available and may facilitate more rapid comprehensive radiographic and/or surgical evaluation. In this case patient had air enema reduction within 3 hours of ED attendance.
There is an excellent article on US for Intussusception by ACEP here.[2] The very basics are covered below.
The “lawn-mower” approach can be used and graded compression along the path can help move bowel gas out of the way to better evaluate intestine. The majority of intussusception (i.e ileocolic type) lie on the right side and subhepatic region. Because deep penetration of the ultrasound beam is not necessary in small children, a high-resolution linear transducer (5-10 MHz) can be used to improve the definition of the image. There is usually associated focal tenderness.

This patient was admitted under paediatric surgeons for a trial of a gas enema. Ultrasound at the bedside gave the diagnosis rapidly and safely without any exposure to radiation.
A very recent meta-analysis (not yet in print) showed that history, physical examination and abdominal ultrasound (which itself is a dose of radiation significant in a paediatric population) have very low diagnostic accuracy and POCUS had a sensitivity of 90.9%, specificity 93.8% and positive likelihood ratio of 19.7[1]. It is a quick and safe modality that can be performed easily at the bedside.
[/expandsub1] [/expand]References/Resources:
- Hom J, Kaplan C, Fowler S, Messina C, Chandran L, Kunkov S. Evidence-Based Diagnostic Test Accuracy of History, Physical Examination, and Imaging for Intussusception: A Systematic Review and Meta-analysis. Pediatr Emerg Care. 2020 Sep 15. doi: 10.1097/PEC.0000000000002224. Epub ahead of print. PMID: 32941364.
- Bellman L, Singh M, Pediatric Emergency Ultrasound: Deep Dive on POCUS for Intussusception, ACEP Emergency Ultrasound (online), last accessed 02/03/2021