Ultrasound of the Week #034
Thanks to Dr Ahmed Abdul-Ghani for this case.
Case:
A normally fit and well 63 year old male came to ED due to 24 hours of chest pain, worse on deep breathing, better when sitting forwards. He had no coryzal symptoms nor radiation of pain.
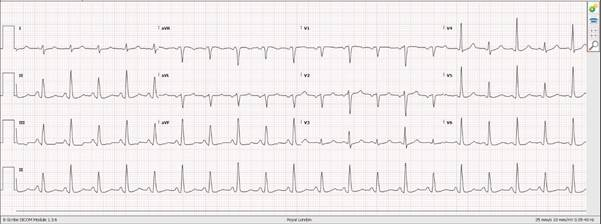
Initially he was taken to the local Cardiac PCI centre with an ECG showing diffuse ST elevation in all leads. This was deemed not to be a STEMI and he sent to the Emergency Department. Troponins were negative.
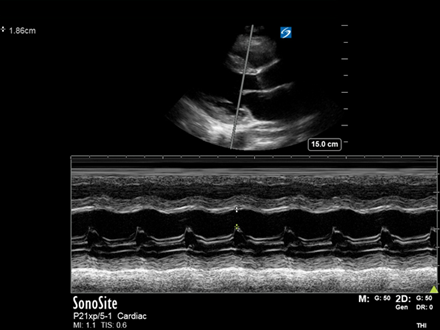
POCUS showed the following:
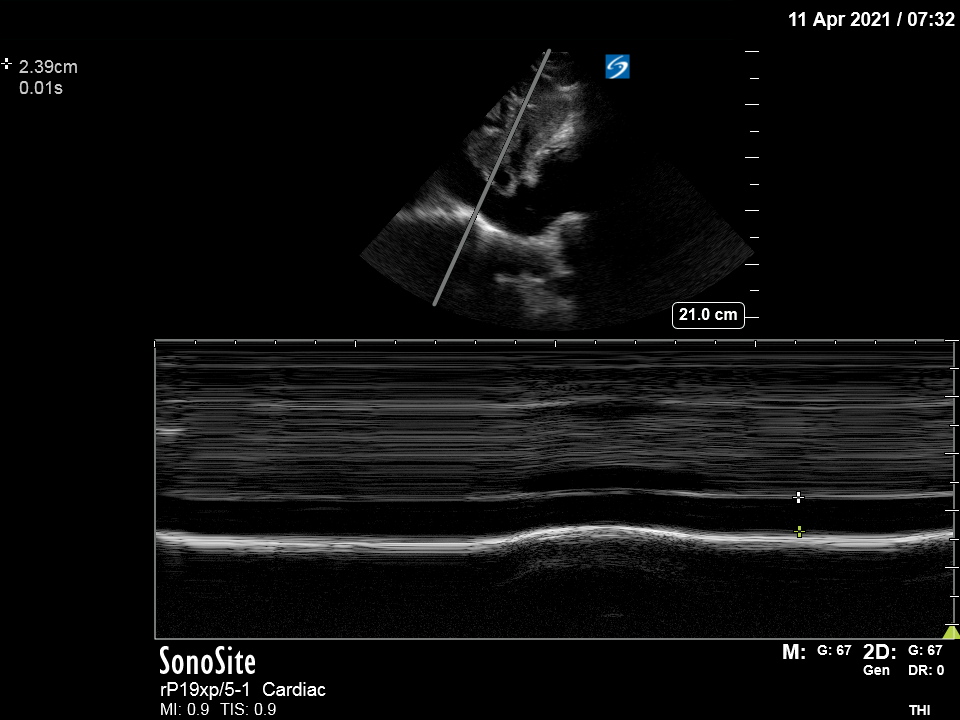
Findings:
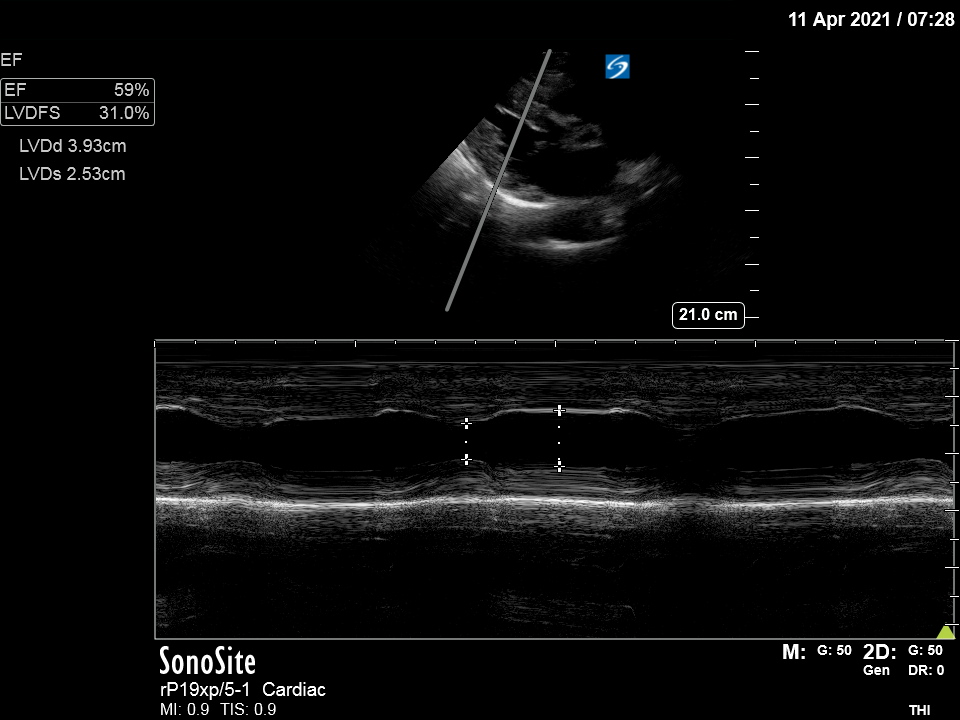
PLAX: Good LVEF (60% on fractional shortening M-mode analysis), hyperechoic pericardium noted with no pericardial effusion.
IVC: 2.39cm with respiratory variation
This is a normal echocardiogram, yet this itself is important information in acute pericarditis (see below).
Echo in Acute Pericarditis:
The European Society of Cardiology (ESC) recommends Transthoracic Echo (TTE) as the first line investigation in suspected pericardial disease, to assess for pericardial effusion +/- tamponade and for ventricular dysfunction secondary to myocardial involvement.[1] For patients with effusions, images should be stored with measurements of effusion to enable follow up studies.
Some studies have demonstrated that up to 60% of patients with pericarditis may have mild-moderate pericardial effusions, with around 5% shown to have signs of cardiac tamponade. The presence of pericardial effusion is a poor prognostic marker in acute pericarditis and so even a basic focused bedside echo assessing for presence/absence of effusion has an important role in risk stratification.
Given the above normal echo, this patient was safely discharged from ED with no follow up.
There is an excellent review on pericarditis on RCEMLearning[2].
Left Ventricular Fractional Shortening:
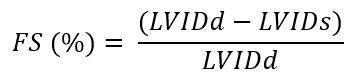
‘Fractional shortening’ (FS) describes the change in LV internal diameter (LVID) from end-diastole (LVIDd) and end-systole (LVIDs)[3]. It is a simple method used to estimate ejection fraction and uses the Teicholz formula to estimate LV volumes and hence ejection fraction. The Teicholz formula is calculated by the Ultrasound machine, giving an estimated Ejection Fraction %, and the details of it need not be remembered.
It is important to note FS is estimating an EF from a single diameter measurement and hence is subject to significant limitations. Various criteria must be met for it to be interpretable:
-LV geometry must be normal, with no regional wall motion abnormalities
-LV electrical activation must be normal (no LBBB)
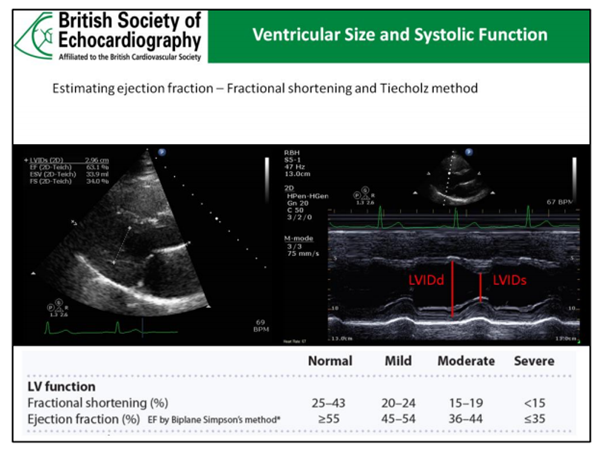
A FS <25% estimates a reduced EF whilst a FS >43% suggests a hyperdynamic LV (often associated with hypovolaemia).
In summary, LV FS is a quick and easy measurement that correlates reasonably well with LVEF if the above criteria are met. However, visual estimation of LVEF has also been shown to correlate well with quantitative FS assessment and is often sufficient in the Emergency Department setting[4].
References:
- Yehuda Adler et al, ESC Scientific Document Group, 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)
Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS), European Heart Journal, Volume 36, Issue 42, 7 November 2015, Pages 2921–2964, https://doi.org/10.1093/eurheartj/ehv318 - Dare L, Pericarditis. RCEMLearning 12/11/2018, available at rcemlearning.co.uk/reference/pericarditis/
- Seif D, Perera P, Mailhot T, Riley D, Mandavia D. Bedside ultrasound in resuscitation and the rapid ultrasound in shock protocol. Crit Care Res Pract. 2012;2012:503254. doi: 10.1155/2012/503254. Epub 2012 Oct 24. PMID: 23133747; PMCID: PMC3485910.
- Weekes AJ, Tassone HM, Babcock A, Quirke DP, Norton HJ, Jayarama K, Tayal VS. Comparison of serial qualitative and quantitative assessments of caval index and left ventricular systolic function during early fluid resuscitation of hypotensive emergency department patients. Acad Emerg Med. 2011 Sep;18(9):912-21. doi: 10.1111/j.1553-2712.2011.01157.x. PMID: 21906201.