Ultrasound of the Week #003
This week’s images combine some basic findings from abdominal ultrasound with the more advanced technique of Ocular Nerve Sheath Diameter. Thanks to Dr Salman Naeem (Ultrasound Fellow) for this case and images.
Case:
These images are from a 55 year old lady who presented with reduced GCS worsening over the previous 3 days. She was known to have some liver disease and was taking methadone.
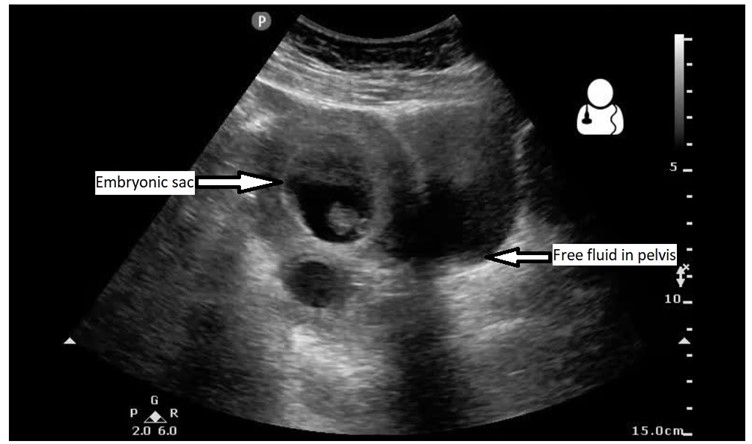
This is a RUQ view of the abdomen – what can you see?

This shows a craggy-edged small liver with free fluid in Morrison’s pouch. In the context of the history, this likely represents ascites secondary to cirrhosis.
[/expand]These are ocular ultrasounds of both eyes:
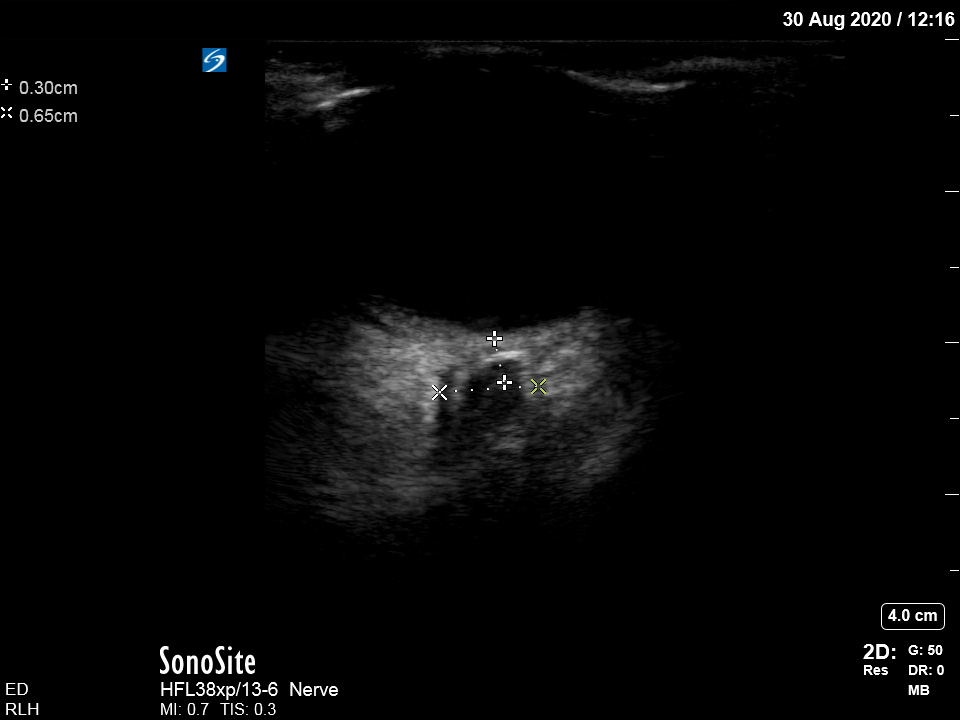
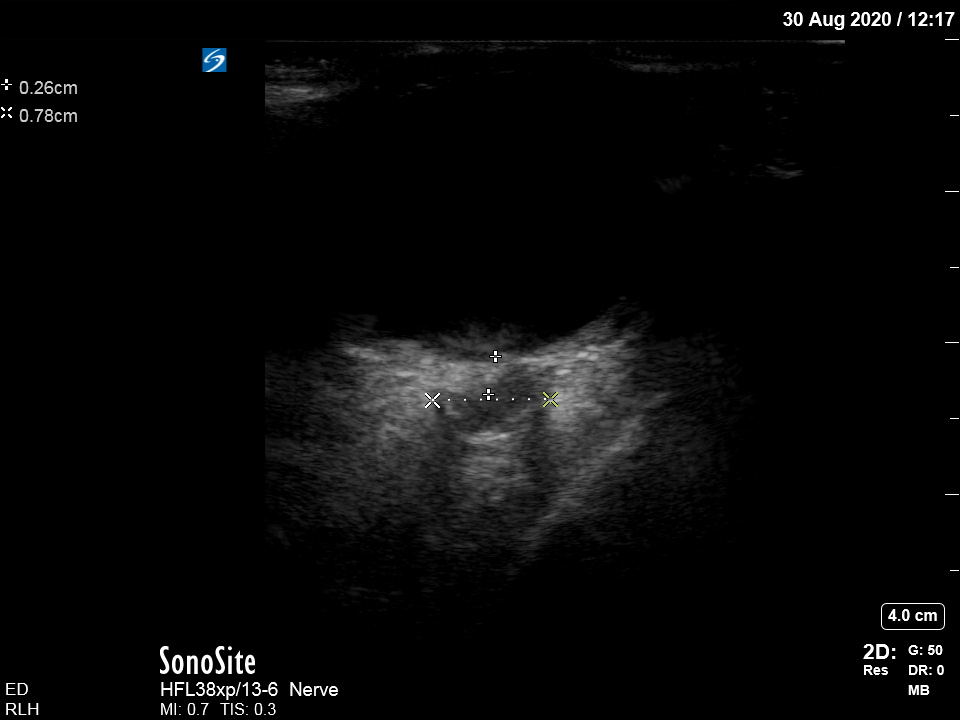
These show an increased Optic Nerve Sheath Diameter (ONSD). The ONSD is measured 3mm posterior to the optic disc and a normal size is <5mm, with an ONSD >6mm suggestive of raised ICP. These images clearly suggest raised ICP, which may be due to hepatic encephalopathy.
[/expand]Lower abdomen and suprapubic :
What do these show?

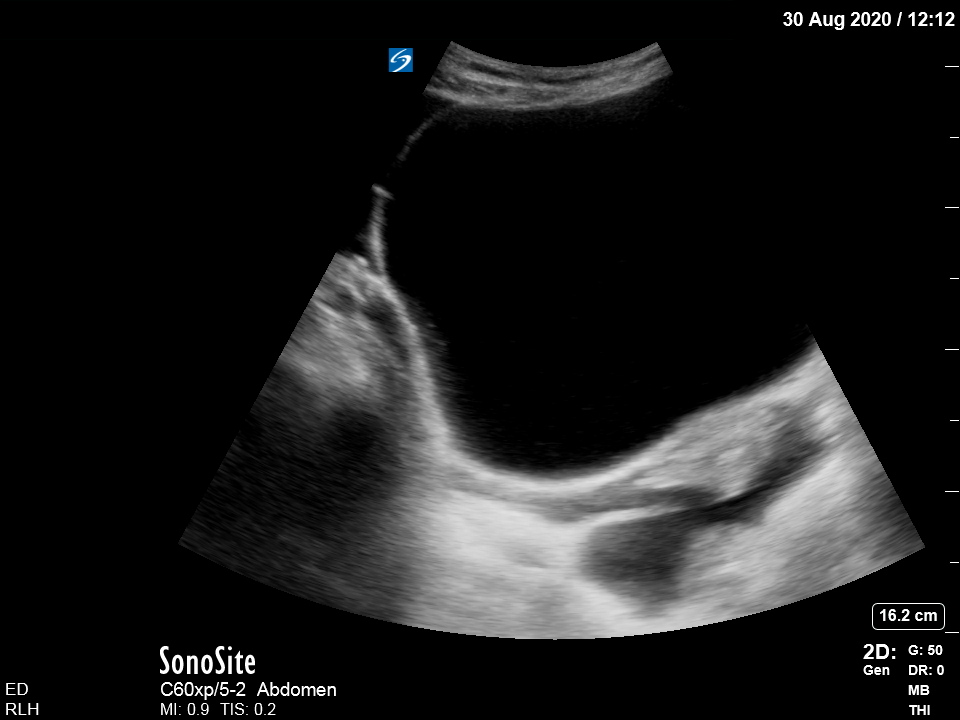
[expand title=”Answer” tag=”h2″]
The abdominal view shows free peritoneal fluid along with bowel loops containing faecal matter. Reduced bowel motions predispose to worsening encephalopathy which is usually treated with laxatives.
The bladder view shows free fluid around the bladder with some loops of bowel present posteriorly.
[/expand]
[expand title=”A bit of an overview of FAST & EFAST Scan:” tag=”h2″]
Focussed Assessment with Sonography for Trauma (FAST) is one of the core RCEM Level 1 Ultrasound skills. The aim is to identify intra-peritoneal free fluid (assumed to be blood in the context of trauma), in order to aid decision making. EFAST (‘Extended FAST’) includes the assessment for pneumothorax. It serves as a good basic skill upon which to learn more complex abdominal, cardiac and thoracic ultrasound.
The EFAST views:
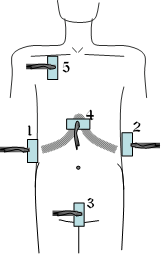
- RUQ : Identifies free fluid in Morrison’s pouch, as well as right sided pleural effusion/haemothorax. (In the supine patient this is the usually the most common site of free fluid accumulation.)
- LUQ : Free fluid around spleen/reno-splenic angle, +left sided pleural effusion/haemothorax
- Suprapubic : Free fluid around the bladder
- Sub-xiphoid : to identify pericardial free fluid
- ‘EFAST’ : to look for lung sliding indicating the ‘lung is up’. Absence has a 86-98% sensitivity & 97-100% specificity for pneumothorax (considerably better than CXR!)
A summary of important points are:
- FAST is only validated in trauma. This doesn’t mean you can’t use ultrasound to identify free fluid from other causes e.g ectopic/ascites (as in the above case), but this is no longer technically a ‘FAST scan’.
- A ‘negative FAST’ is not sufficient to exclude intra-abdominal free fluid. It is a ‘rule-in’ not ‘rule-out’ test.
- It is not sufficient to rule out visceral injury – CT remains gold standard.
- In the first world with good access to trauma CT, a FAST is only indicated in a haemodynamically unstable trauma patient who may need to go straight to theatre.
- FAST doesn’t mean it needs to be done fast! (Although in the context of trauma, it should be done by an experienced scanner who can do it quickly.
There are excellent learning resources on RCEMLearning : https://www.rcemlearning.co.uk/modules/introduction-to-ultrasound-physics-and-the-role-of-fast-scanning-in-the-ed/
A great video of EFAST scanning is found here from ‘5-minute Sono’ : https://www.youtube.com/watch?v=2VtrOAbqBsw
[/expand]