HEMS Teams should perform a two-point examination bilaterally in the most anterior portion of the chest (depending on patient position) evaluating for presence or absence of lung sliding to answer the question:
- Is there a pneumothorax?
This investigation is likely to be useful in the following scenarios:
- The awake patient with trauma to the thorax, not in extremis, to increase diagnostic accuracy and would usually be performed while en-route to hospital.
- The intubated patient where there has not been a clear indication to proceed to thoracostomies. POCUS can aid in this decision making and may be done on scene (if it will prompt or change this decision), alternatively, may be done while en-route to hospital to identify or monitor chest disease progression.
- The intubated patient without thoracostomies that has become haemodynamically unstable or difficult to ventilate, to aid with diagnosing the cause of shock/ ventilation difficulty and to direct treatment.
Obtaining the View
Use the linear OR abdominal probes for viewing ribs and pleural disease i.e., pneumothorax and pleural effusions.
Set the depth to 5cm. Place the probe vertically in the most anterior (least dependent) area of the thorax, with the marker toward the head. In the supine position this will be the anterior thorax around the 2nd – 3rd intercostal space. Visualise the rib shadows at the lateral sides of the screen with the pleura (bright line between ribs) positioned centrally. Look for the presence or absence of lung sliding.
Interpreting the View
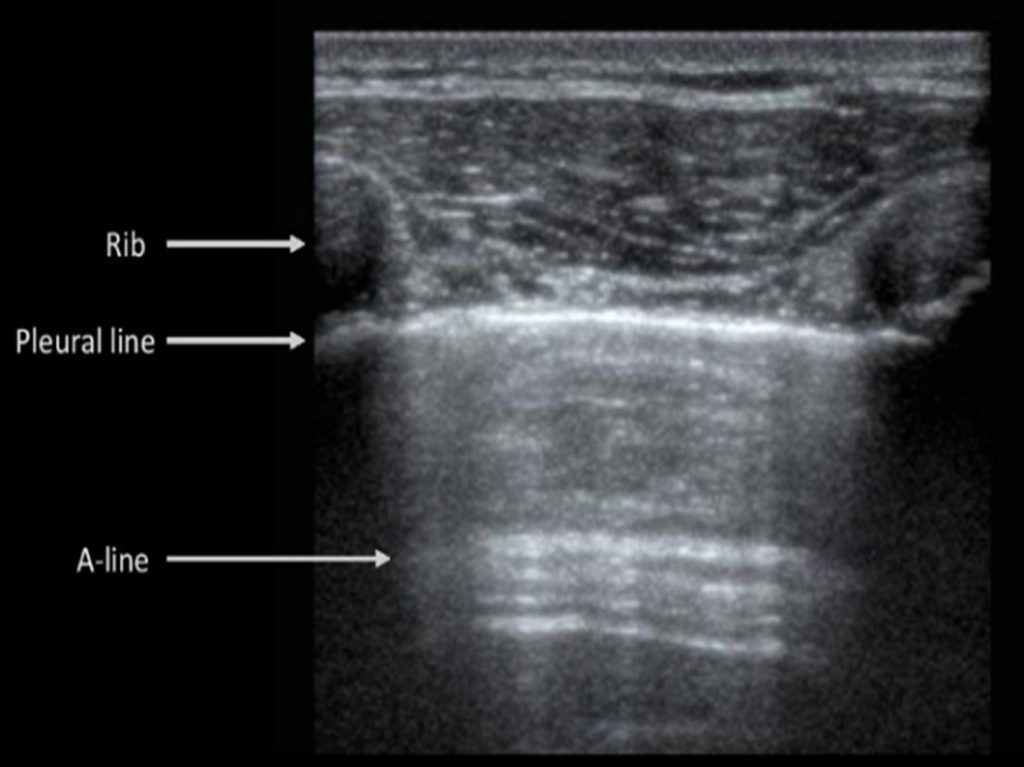
Lung ultrasound images consist of both directly visualized chest structures and ultrasound artifacts that require careful interpretation. Chest wall structures are seen at the top of the screen above the bright pleural line. Below the pleural line, the alveolar air content of the lung creates an acoustic interface with the pleura and the soft tissues of the chest wall preventing visualisation of a direct view of the lung parenchyma. Instead, lung tissue is represented by ultrasound artifacts that have characteristic significance.
A-lines: Horizontal hyperechoic (white) lines at constantly spaced intervals below the pleura due to reverberations between the pleura and the ultrasound probe. They represent well aerated lung and are seen in normal lung, asthma/ COPD and pneumothorax.
B-lines: Reverberation artefacts which originate from the pleura and continue to the bottom of the screen like search lights. They represent increased lung density. Their further interpretation is beyond the scope of this document, but their presence rules out pneumothorax. They are also known as ‘Comet tails.
Lung sliding: A horizontal rhythmic movement of the pleural line in synchronization with respiration. This is often described as a ‘shimmering’ or ‘marching ants’ pattern and the presence of lung sliding indicates that the lung is ventilating in the inspected area.
Pneumothorax is diagnosed by the combination of absence of lung sliding and absence of B-lines (Comet tails). Be aware that lung sliding may also be absent in patients with respiratory arrest, pleural adhesions and in mainstem bronchial intubation.
Video Review: