Ultrasound of the Week #027
Many thanks to Dr Tom Chambers, FY2 for this great case.
Case:
A 34 year old male smoker with no other PMH presented with left sided sharp chest pain and shortness of breath. He had had COVID-19 some weeks before and yet had recovered well, managing to go back to work although had continued to be easily fatigued and breathless with strenuous activity. He also reported 2 weeks of left calf pain.
With ambulance crew SpO2 was 70% and 93% on 15L NRBM. ECG showed RBBB, sinus tachycardia.
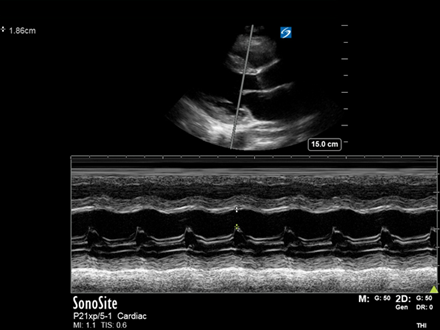
A bedside echo was performed showing the following:
Question: What does this show?
Answer: There are some interesting findings here that may not be immediately apparent.
The LV is not small/dilated. Contractility of the lateral base (above the MV) appears good, yet on closer inspection is the only LV wall that really seems to be contracting well.
Whilst the IVS is moving in towards the LV, it isn’t thickening appropriately and is thinned, being pushed into the LV (rather than thickening into both ventricles). Looking closely at the LV apex, a large thrombus can be seen sitting there which is hardly moving.
The RV is not dilated and a visual TAPSE seems to indicate good longitudinal function.
The IVS & LV apex are supplied by the LAD and this gentleman has clearly had an LAD MI in the past (not acutely as the walls are thinned), causing septal/apical akinesia and allowing the formation of an LV thrombus.
Case Progression:
A CTPA showed a saddle PE with extension into the lobar arteries. Point-of-care troponin was 24. He was given half-dose thrombolysis (50mg) in A&E and admitted to Intensive Care for post-op care.
A departmental echo was performed the following day reported as follows:
This was a technically difficult study with some suboptimal views due to habitus.3. Non-dilated LV. The LV apex through to mid anterolateral segments are thin walled and aneurysmal. Near all segments appear either akinetic or with a significant degree of impairment. Overall EF appears <15%.
4. Dilated RV with impaired function
5. Mildly dilated LA
6. No obvious, significant valvular abnormalities detected
7. There is a large thrombus seen in the apical anteroseptal/apical region of the LV measuring approx 4.3cm x 1.7cm.
His RV function had deteriorated between his ED focused echo and his departmental echo, even with thrombolytic therapy.
Sadly a few days later he was noted to have facial droop and reduced GCS and diagnosed with an ischaemic CVA, undergoing mechanical thrombectomy the same day.
LV thrombus is a recognised complication of acute myocardial infarction although is now much less common since the introduction of primary PCI[1]. It can occur some time after the initial event and is more common in those with significantly reduced LVEF and significant RWMAs[3]. Standard treatment is anticoagulation with warfarin although DOACs are now being used in various cases[2]. Data on thrombolysis as a treatment is very limited and systemic embolic complications remain a risk with or without treatment, with the 1 year ischaemic stroke risk being 10%[3].
Thrombolysis is the accepted treatment in acute massive PE with hypotension or cardiogenic shock. However, there is much debate about the utility of thrombolytics in the management of sub-massive PE and robust RCT data is limited[4]. Whilst some studies suggest higher rates of significant bleeding with thrombolysis vs heparin, others suggest that we should be utilising RV strain assessment and/or reduced dose thrombolytic regimens to optimise individual patient care[5,6]. There is an excellent article on sub-massive PE management at pulmcrit here.
Verified by Dr Behnaz Mahmoodian, MD, FRCEM, PGCert US, Lead for Emergency Ultrasound, Royal London Hospital.
References:
- Keren A, Goldberg S, Gottlieb S, Klein J, Schuger C, Medina A, Tzivoni D, Stern S. Natural history of left ventricular thrombi: their appearance and resolution in the posthospitalization period of acute myocardial infarction. J Am Coll Cardiol. 1990 Mar 15;15(4):790-800. doi: 10.1016/0735-1097(90)90275-t. PMID: 2307788.
- Robinson AA, Trankle CR, Eubanks G, Schumann C, Thompson P, Wallace RL, Gottiparthi S, Ruth B, Kramer CM, Salerno M, Bilchick KC, Deen C, Kontos MC, Dent J. Off-label Use of Direct Oral Anticoagulants Compared With Warfarin for Left Ventricular Thrombi. JAMA Cardiol. 2020 Jun 1;5(6):685-692. doi: 10.1001/jamacardio.2020.0652. PMID: 32320043; PMCID: PMC7177639.
- Ali, Z., Isom, N., Dalia, T. et al. Direct oral anticoagulant use in left ventricular thrombus. Thrombosis J 18,29 (2020). https://doi.org/10.1186/s12959-020-00242-x
- Goldhaber SZ. Thrombolysis in pulmonary embolism: a large-scale clinical trial is overdue. Circulation. 2001 Dec 11;104(24):2876-8. PMID: 11739298.
- Aykan AC et al. Low dose prolonged infusion of tissue type plasminogen activator therapy in massive pulmonary embolism. European Heart J 2014; 35(Suppl 1): 69.
- Farkas J, Submassive PE 2017: Getting ’em off the cliff Available at https://emcrit.org/pulmcrit/submassive-pe-peitho/, last accessed 02/04/2021