Ultrasound of the Week #026
Special thanks to Dr Behnaz Mahmoodian, Emergency Department US Lead for this great and unusual case.
Case:
A 74 year old male with a PMH of angina, CKD3, COPD and diverticulitis presented with a 1 week history of abdominal pain and 1 day of confusion.
Initial obs in the ED were: SpO2 98%, FiO2 0.35, T36, BP152/83, HR76, RR24
Whilst in A&E he developed a progressive oxygen requirement and worsening confusion and was in significant abdominal discomfort.
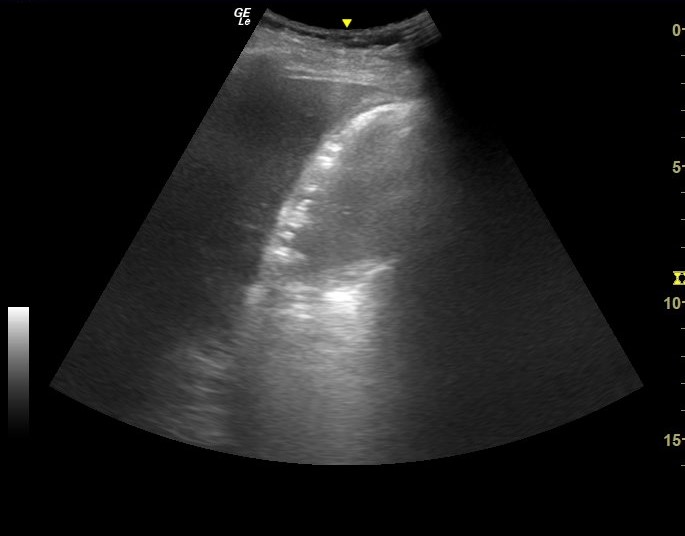
A POCUS of his RUQ showed the following:
Question: What organ is this and what is the diagnosis?
Answer:
This is the gallbladder. The liver is seen to the left of the screen and the gallbladder brightly (too brightly!) outlined in the centre. This is emphysematous cholecystitis, which has a mortality rate of 15-25%, compared to <5% for uncomplicated cholecystitis.[1]
The highly echogenic walls with low level reverberation artefact are highly predictive of gas in the gallbladder wall. Another sign that may be seen is small echogenic foci ‘floating’ up through the wall (bubbles of gas), which are highly specific for gas and can also be seen in the liver in cases of pneumobilia.
Note – air seen inside the gallbladder itself following ERCP or papillotomy should not be mistaken for emphysematous cholecystitis!
Case Progression:
This patient was admitted to intensive care and underwent a percutaneous cholecystotomy the following day. In this case, the POCUS was performed not long after the patient’s arrival, almost 10 hours before his CT scan was reported, rapidly expediting his diagnosis.
References:
- Vadera, Radswiki et al. Emphysematous Cholecystitis. Radiopedia, accessible at https://radiopaedia.org/articles/emphysematous-cholecystitis. Last accessed 26/03/2021