Ultrasound of the Week #012

Thanks to Dr Behnaz Mahmoodian for this interesting case and great images.
Case:
A painter/decorator in his 40’s presented with a week’s history of shortness of breath, non-productive cough and palpitations. He had no chest pain, fever, change in smell/taste, no known COVID/TB infected contacts and no recent travel.
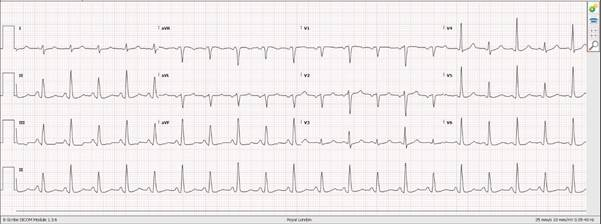
He was found to be in Atrial Fibrillation and chest XR showed bilateral lower opacifications that were not clearly distinguishable between consolidation or pleural effusions.
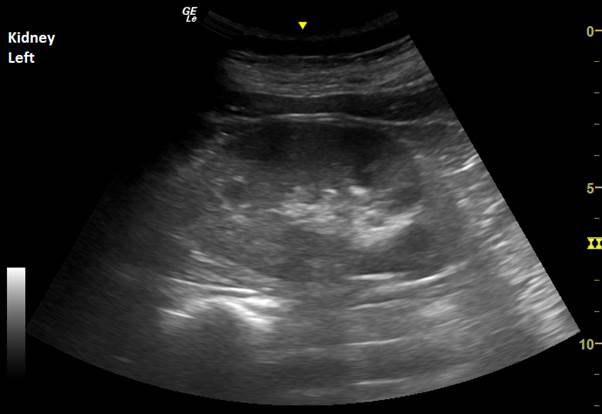
Bedside lung, cardiac and abdominal ultrasound was performed to provide further diagnostics.
Answers:
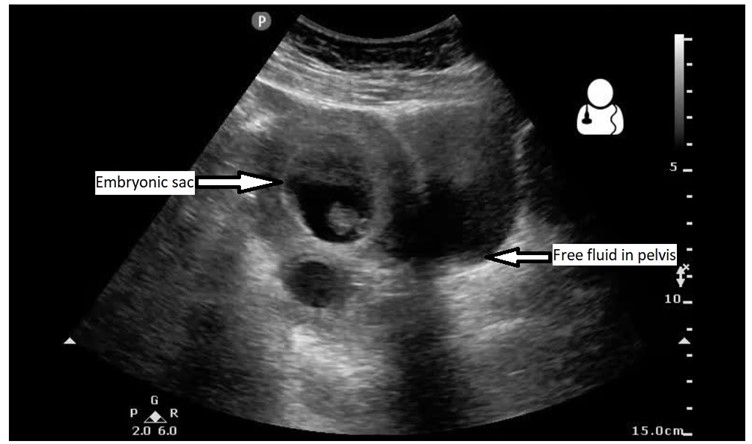
You can see some rather unusual things in his chest (remember – you shouldn’t be able to see anything but lung artifact!) There are bilateral effusions, with the left slightly larger than the right. The right contains a large septated collection – this is an empyema. In the LUQ view you can clearly see free pertioneal fluid above the spleen.
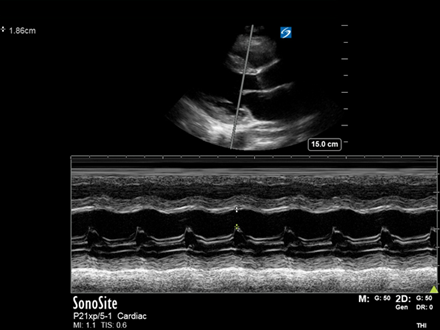
Echo showed significant biventricular impairment.
This gentleman had a CT showing ‘multifocal spiculated nodules predominantly in the upper lobes, with associated cavitation highly suspicious for TB. Other atypical infection could also be included in the differential. The right pleural collection with associated pleural thickening is consistent with an empyema.’
He was admitted under the medical team and investigated for his seemingly acute heart failure, lung lesions and abdominal free fluid (remember free abdominal fluid in TB may be peritoneal TB).
Lung Ultrasound for Pleural fluid:
Lung ultrasound is an extremely useful skill for the Emergency Physician and can assess a large range of pathologies including pneumothorax, pneumonia and rib fractures, amongst others. We will cover a range of different uses of Lung Ultrasound in following cases.
Pleural effusions:
Lung ultrasound has a similar sensitivity and specificity to CT for pleural effusions, with the advantage that ultrasound can often distinguish transudate from exudate. Under normal conditions lung is aerated and therefore does not well conduct ultrasound. We can use this to our advantage in identifying pleural/pulmonary pathology. Since fluid is hypoechoic (dark) this is usually easily recognised and most commonly seen at the posterolateral point. Effusions are best assessed with the patient sat up and leaning over a table/pillow, as seen below. If this is not possible, fluid will collect most posteriorly and so a posterolateral view (akin to a more cephalad RUQ/LUQ FAST view) will likely demonstrate an effusion if present and can indeed be utilised in trauma to identify haemothorax.
Fluid can be assessed for:
- estimated volume
- signs of transudate vs exudate
- signs of associated pathology (consolidation, collapse, pulmonary oedema)
Ultrasound is also invaluable (and now considered standard of care) for pleural procedures such as therapeutic aspiration and chest drain insertion.
References:
- Mayo PH, Copetti R, Feller-Kopman D, Mathis G, Maury E, Mongodi S, Mojoli F, Volpicelli G, Zanobetti M. Thoracic ultrasonography: a narrative review. Intensive Care Med. 2019 Sep;45(9):1200-1211. doi: 10.1007/s00134-019-05725-8. Epub 2019 Aug 15. PMID: 31418060.
- Reissig A, Copetti R, Kroegel C. Current role of emergency ultrasound of the chest. Crit Care Med. 2011 Apr;39(4):839-45. doi: 10.1097/CCM.0b013e318206d6b8. PMID: 21263325.