Ultrasound of the Week #008
Thanks to Dr Serena Rovida, Emergency Medicine SpR for this great case and images.
Case:
A male in his early twenties presented with severe abdominal pain, nausea and vomiting present for 2 days.
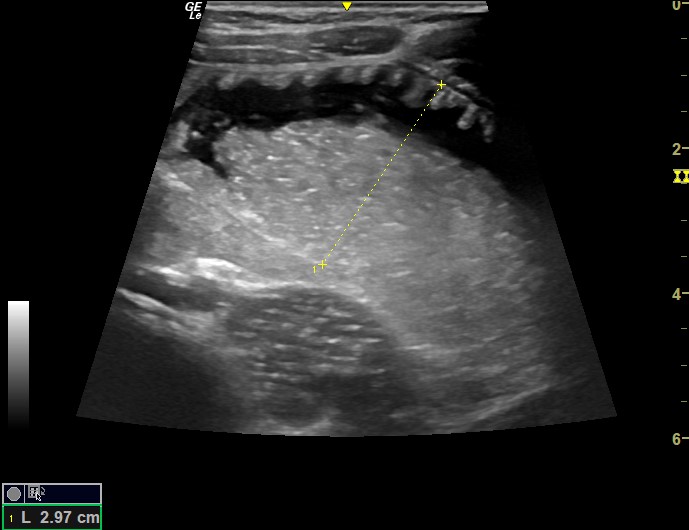
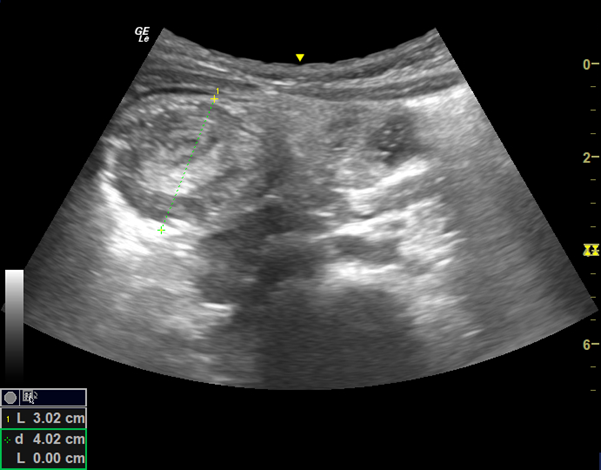
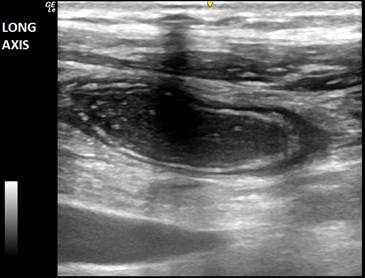
A bedside ultrasound of his lower abdomen was performed showing the following images:
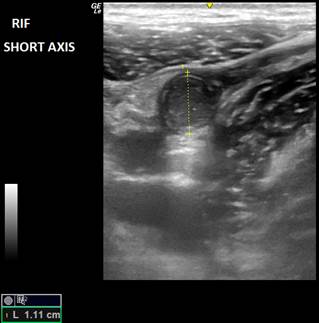
Question 1: What does it show?
[expand title=”Answer 1: ” tag=”h3″] This shows a dilated, non-compressible appendix >6mm (diagnostic for appendicitis). [/expand]
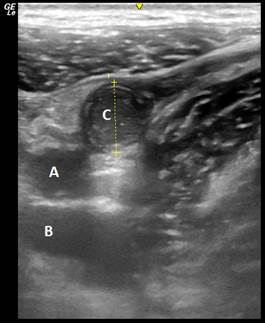
Question 2: What are the structures A, B and C?
[expand title=”Answer 2: ” tag=”h3″] A: Iliac artery (non-compressible) B: Iliac vein (compressible) C: Appendix.
This patient was rapidly referred to surgeons and admitted for appendicectomy. [/expand]<br>
[expand title=”Point-of-Care-Ultrasound for Appendicitis:” tag=”h2″ trigclass=”noarrow”]
POCUS can be used to identify acute appendicitis in patients with moderate to high pre-test probability.[1] A high specificity yet lower sensitivity make it a rule-in but not a rule-out test (not to be used as a screening tool). As the appendix can vary significantly in position, it is not uncommon to be difficult or impossible to locate.
Technique:
-Graded compression to mobilise the overlying gas
-The classic approach is sweeping the entire RLQ with a ‘lawnmower’ technique [2]

Summary of Findings:
Acute appendicitis:
- Much easier seen when abnormal: blind-ended tubular structure, overlying psoas muscle and iliac vessels, with thickened walls, >7mm( outer diameter) considered abnormal (6mm cut-off may lead to high sensitivity and lower specificity[3]).
- Surrounded by inflamed mesenteric fat: bright echogenic area +/- few lymph nodes
- Thickened wall with well demarcated mucosal layers due to oedema
- False negatives: missing tip appendicitis
- False positives: inflammation secondary to other intra-abdominal processes (Crohn’s, PID, etc.)
Secondary signs:
- Sonographic McBurney’s: selective compression over suspected structure causing pain
- Appendicolith: highly suggestive, echogenic structure with post-acoustic shadow
- Wall hyperaemia with loss of definition at later stages
- Thickened bright echogenic mesenteric fat
- Mesenteric lymph nodes
- Free fluid wedges or larger focal fluid in the RLQ or diffuse in case of perforation
- Ileus
- Collection
Mimics:
- Terminal ileum/small bowel (normal)
- Terminal ileitis
- Mesenteric adenitis: 3-5 lymph nodes >5mm in diameter but no other secondary signs
- Ovarian pathology
- Meckel’s diverticulum: cystic structure (rare)
[/expand]
References:
- Fields MJ, Davis J, Alsup C, et al. Accuracy of point-of-care ultrasonography for diagnosing acute appendicitis: a systematic review and meta-analysis.Acad Emerg Med. 2017;24(9):1124-36.
- Sivitz AB, Cohen SG, Tejani C. Evaluation ofacute appendicitis by pediatric emergency physician sonography.Ann Emerg Med 2014; 64(358–64): e4.
- H P Chicaiza, L Malia, C H Mulvey, S R Smith.Revisiting the Appendiceal Diameter via Ultrasound for the Diagnosis of Acute Appendicitis, Pediatr Emerg Care. 2018 Nov;34(11):757-760
- Benabbas R, Hanna M, Shah J, et al. Diagnostic accuracy of history, physical exam, laboratory tests and point-of-care-ultrasound for pediatric acute appendicitis in the emergency department: a systematic review and meta-analysis.Acad Emerg Med. 2017;24(5):523-51.